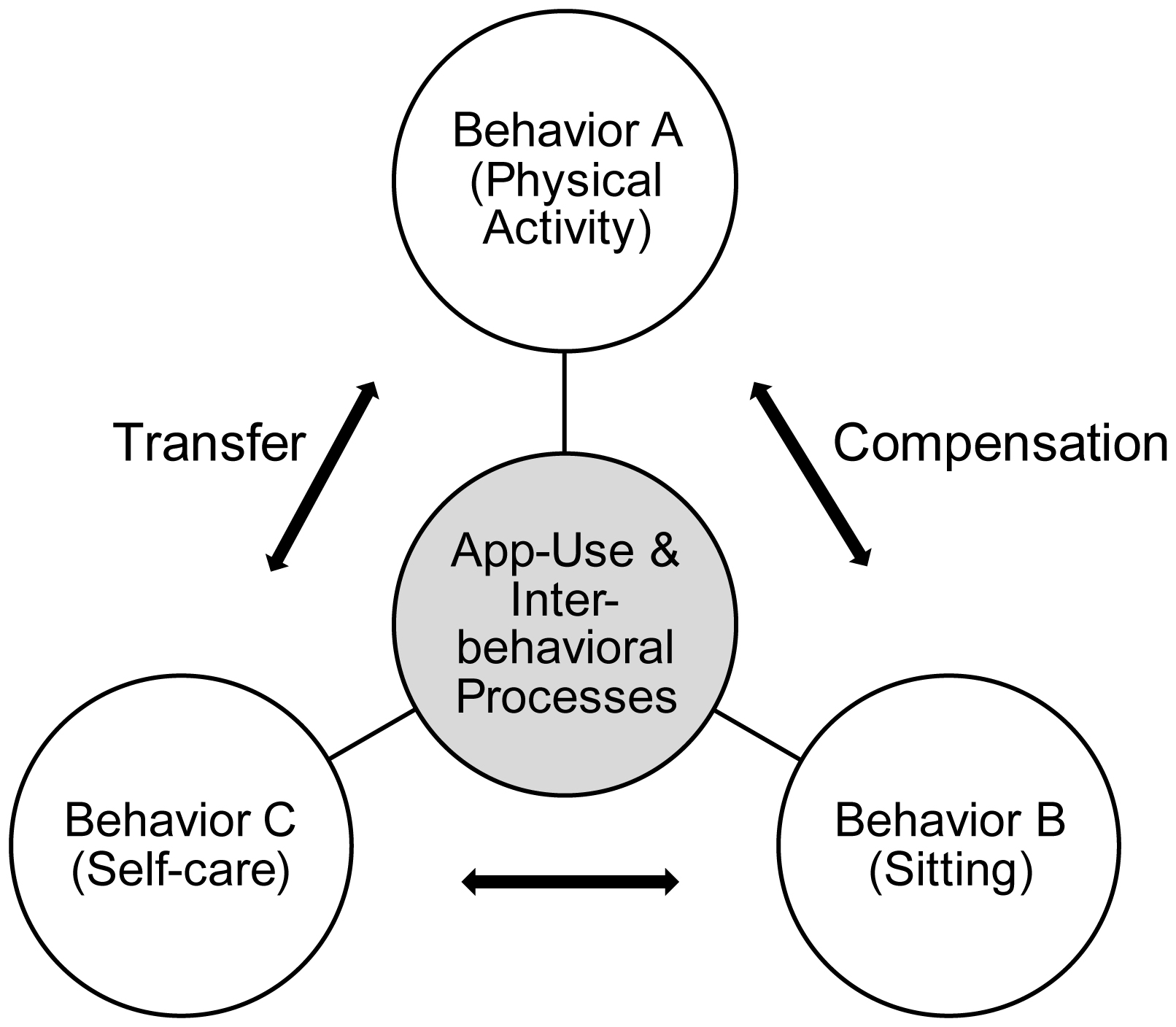
Prevention of acute cardiovascular events in patients with cardiovascular disease (CVD) requires promoting health-protective behaviors (e.g., physical activity) and reducing health-compromising behaviors (e.g., sitting). Digital interventions addressing health behavior offer great potential. Based on a multiple behavior change theory, an intervention in the form of a digital health application (app) was evaluated in a pilot trial, testing the following hypotheses (H): H1: Health behaviors (physical activity, sitting) and disease self-management (self-care maintenance, self-care confidence) are closely related; H2: changes in health behaviors and disease self-management indicators over time (T0 to T1) are more pronounced in the intervention group (IG, app users) than in the control group (CG); H3: within the IG, changes in systolic and diastolic blood pressure indicate a positive trajectory.
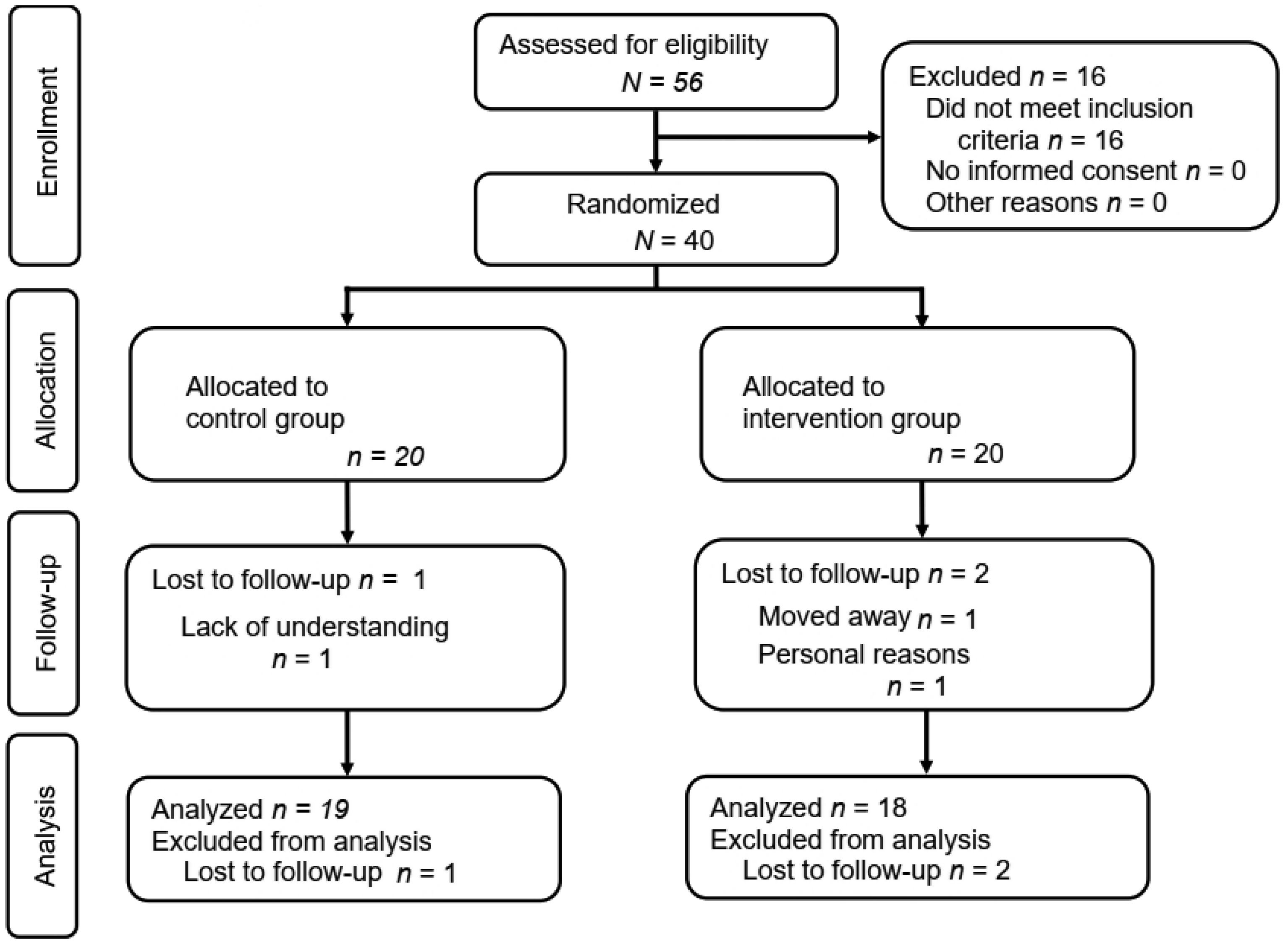
A 12-week randomized controlled trial (RCT) was conducted with two measurement points. The IG received an app addressing self-management and health behavior change. A total of N = 40 CVD patients were randomized equally to the CG (45% women; mean age = 60.6 years) and the IG (35% women; mean age = 61.5 years).
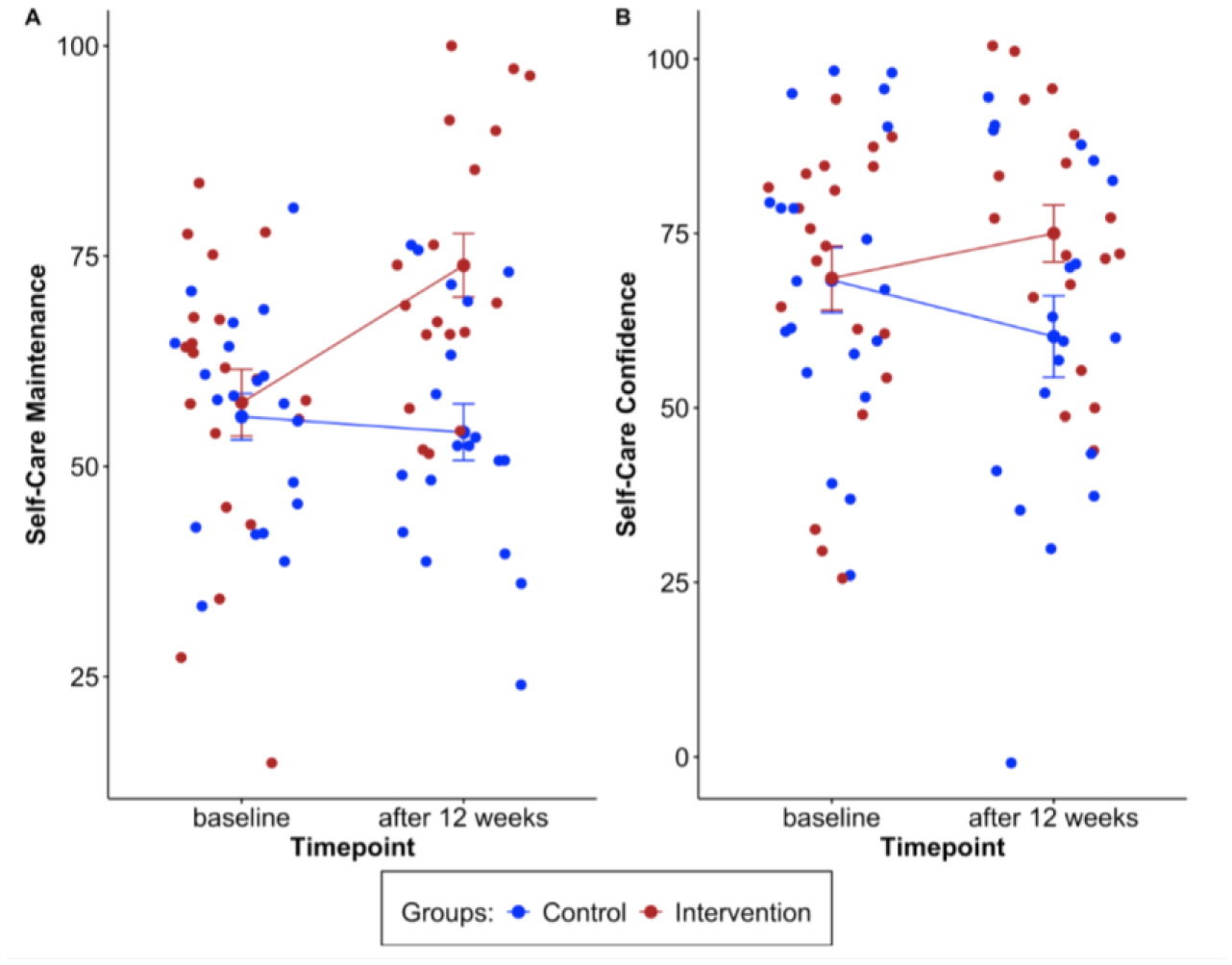
Findings support H1 with correlations between behaviors (r = −0.66–0.79) and disease self-management (r = −0.06–0.70). H2 was also partially supported, with significant improvements over time in self-management indicators, especially self-care maintenance, in the IG (Eta² = 0.35; p < 0.001). H3 could not be confirmed as no significant changes were found.
This study provides evidence that an app addressing different behavior change techniques (BCTs) can help to manage CVD by promoting health-protective behaviors and preventing health-compromising behaviors. Taking different behaviors into account may increase the effectiveness of behavioral intervention, thereby improving individual and public health. Replications with larger samples and more objective measures are needed.
Citation: Sonia Lippke, Luisa Korte, Vinayak Anand Kumar, Andreas Fach, Tiara Ratz. Health behavior and disease self-management indicators in patients with cardiovascular diseases using a health app: Findings from an RCT[J]. AIMS Public Health, 2025, 12(1): 233-258. doi: 10.3934/publichealth.2025015
Prevention of acute cardiovascular events in patients with cardiovascular disease (CVD) requires promoting health-protective behaviors (e.g., physical activity) and reducing health-compromising behaviors (e.g., sitting). Digital interventions addressing health behavior offer great potential. Based on a multiple behavior change theory, an intervention in the form of a digital health application (app) was evaluated in a pilot trial, testing the following hypotheses (H): H1: Health behaviors (physical activity, sitting) and disease self-management (self-care maintenance, self-care confidence) are closely related; H2: changes in health behaviors and disease self-management indicators over time (T0 to T1) are more pronounced in the intervention group (IG, app users) than in the control group (CG); H3: within the IG, changes in systolic and diastolic blood pressure indicate a positive trajectory.
A 12-week randomized controlled trial (RCT) was conducted with two measurement points. The IG received an app addressing self-management and health behavior change. A total of N = 40 CVD patients were randomized equally to the CG (45% women; mean age = 60.6 years) and the IG (35% women; mean age = 61.5 years).
Findings support H1 with correlations between behaviors (r = −0.66–0.79) and disease self-management (r = −0.06–0.70). H2 was also partially supported, with significant improvements over time in self-management indicators, especially self-care maintenance, in the IG (Eta² = 0.35; p < 0.001). H3 could not be confirmed as no significant changes were found.
This study provides evidence that an app addressing different behavior change techniques (BCTs) can help to manage CVD by promoting health-protective behaviors and preventing health-compromising behaviors. Taking different behaviors into account may increase the effectiveness of behavioral intervention, thereby improving individual and public health. Replications with larger samples and more objective measures are needed.

| [1] |
Abell B, Glasziou P, Hoffmann T (2017) The contribution of individual exercise training components to clinical outcomes in randomised controlled trials of cardiac rehabilitation: A systematic review and meta-regression. Sports Med Open 3: 19. https://doi.org/10.1186/s40798-017-0086-z 
|
| [2] |
Coccia M, Benati I (2024) Negative effects of high public debt on health systems facing pandemic crisis: Lessons from COVID-19 in Europe to prepare for future emergencies. AIMS Public Health 11: 477-498. https://doi.org/10.3934/publichealth.2024024
|
| [3] |
Schmid T (2015) Costs of treating cardiovascular events in Germany: A systematic literature review. Health Econ Rev 5: 27. https://doi.org/10.1186/s13561-015-0063-5
|
| [4] |
Townsend N, Kazakiewicz D, Lucy Wright F, et al. (2022) Epidemiology of cardiovascular disease in Europe. Nat Rev Cardiol 19: 133-143. https://doi.org/10.1038/s41569-021-00607-3
|
| [5] |
Montalva-Valenzuela F, Castillo-Paredes A, Farias-Valenzuela C, et al. (2024) Effects of exercise, physical activity, and sports on physical fitness in adults with down syndrome: A systematic review. AIMS Public Health 11: 577-600. https://doi.org/10.3934/publichealth.2024029
|
| [6] |
Jansson AK, Schumacher TL, Kocanda L, et al. (2024) A systematic review of the completion of cardiac rehabilitation programs for adults aged 18–50 years. J Cardiopulm Rehabil Prev 44: E30-E51. https://doi.org/10.1097/HCR.0000000000000881
|
| [7] | Gesundheitsberichterstattung des BundesDeaths (absolute, death rate, ranks, proportions) for the 10/20/50/100 most frequent causes of death (from 1998). Classification features: Years, region, age, sex, ICD-10. [cited 2025 Feb 20th] (2025). Available from: www.gbe-bund.de |
| [8] | Heidemann C, Scheidt-Nave C, Beyer AK, et al. (2021) Health situation of adults in Germany–results for selected indicators from GEDA 2019/2020-EHIS. J Health Monit 6: 3-25. |
| [9] |
Knuuti J, Wijns W, Saraste A, et al. (2020) 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 41: 407-477. https://doi.org/10.1093/eurheartj/ehz425
|
| [10] |
Su J, Xiong J, Ke Q, et al. (2023) Experiences and perceptions of acute myocardial infarction patients with a prolonged decision-making phase of treatment seeking: A meta-synthesis. J Clin Nurs 32: 7891-7908. https://doi.org/10.1111/jocn.16802
|
| [11] |
Su JJ, Liu JYW, Cheung DSK, et al. (2023) Long-term effects of e-Health secondary prevention on cardiovascular health: a systematic review and meta-analysis. Eur J Cardiovasc Nurs 22: 562-574. https://doi.org/10.1093/eurjcn/zvac116
|
| [12] |
Fach A, Osteresch R, Erdmann J, et al. (2020) Long-term prevention after myocardial infarction in young patients ≤45 years: the Intensive Prevention Program in the Young (IPP-Y) study. Eur J Prev Cardiol 27: 2264-2266. https://doi.org/10.1177/2047487319883960
|
| [13] |
Osteresch R, Fach A, Frielitz FS, et al. (2021) Long-term effects of an intensive prevention program after acute myocardial infarction. Am J Cardiol 154: 7-13. https://doi.org/10.1016/j.amjcard.2021.05.034
|
| [14] |
Wienbergen H, Fach A, Meyer S, et al. (2019) Effects of an intensive long-term prevention programme after myocardial infarction–a randomized trial. Eur J Prev Cardiolog 26: 522-530. https://doi.org/10.1177/2047487318781109
|
| [15] |
Fischer C, Höpner J, Hartwig S, et al. (2021) Participation in disease management programs and major adverse cardiac events in patients after acute myocardial infarction: A longitudinal study based on registry data. BMC Cardiovasc Disord 21: 18. https://doi.org/10.1186/s12872-020-01832-3
|
| [16] |
AlHabeeb W (2022) Heart failure disease management program: A review. Medicine (Baltimore) 101: e29805. https://doi.org/10.1097/MD.0000000000029805
|
| [17] |
Sawicki OA, Mueller A, Glushan A, et al. (2020) Intensified ambulatory cardiology care: effects on mortality and hospitalisation—a comparative observational study. Sci Rep 10: 14695. https://doi.org/10.1038/s41598-020-71770-9
|
| [18] |
Grigoriev P, Sauerberg M, Jasilionis D, et al. (2024) Sterblichkeitsentwicklung in Deutschland im internationalen Kontext. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 67: 493-503. https://doi.org/10.1007/s00103-024-03867-9
|
| [19] |
Wing C, Simon K, Bello-Gomez RA (2024) Designing difference in difference studies: Best practices for public health policy research. Annu Rev Public Health 39: 453-469. https://doi.org/10.1146/annurev-publhealth-040617-013507
|
| [20] |
Buss VH, Barr M, Parker SM, et al. (2024) Mobile app intervention of a randomized controlled trial for patients with obesity and those who are overweight in general practice: User engagement analysis quantitative study. JMIR Mhealth Uhealth 12: e45942. https://doi.org/10.2196/45942
|
| [21] |
Liu C, Wang D, Liu C, et al. (2020) What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam Med Com Health 8: e000351. https://doi.org/10.1136/fmch-2020-000351
|
| [22] |
Duan Y, Li X, Guo L, et al. (2022) A Wechat mini program-based intervention for physical activity, fruit and vegetable consumption among Chinese cardiovascular patients in home-based rehabilitation: A study protocol. Front Public Health 10: 739100. https://doi.org/10.3389/fpubh.2022.739100
|
| [23] |
Heimer M, Schmitz S, Teschler M, et al. (2023) eHealth for maintenance cardiovascular rehabilitation: a systematic review and meta-analysis. Eur J Prev Cardiol 30: 1634-1651. https://doi.org/10.1093/eurjpc/zwad145
|
| [24] |
Ulrich S, Gantenbein AR, Zuber V, et al. (2024) Development and evaluation of a smartphone-based chatbot coach to facilitate a balanced lifestyle in individuals with headaches (BalanceUP App): Randomized controlled trial. J Med Internet Res 26: e50132. https://doi.org/10.2196/50132
|
| [25] |
Zhang YB, Pan XF, Lu Q, et al. (2023) Association of combined healthy lifestyles with cardiovascular disease and mortality of patients with diabetes: An international multicohort study. Mayo Clin Proc 98: 60-74. https://doi.org/10.1016/j.mayocp.2022.08.012
|
| [26] |
Reif S, Schubert S, Stiefel J, et al. (2022) Supporting patients with heart failure with digital therapeutics—A pilot study in Germany. Digit Health 8: 205520762211438. https://doi.org/10.1177/20552076221143899
|
| [27] |
Shahaj O, Denneny D, Schwappach A, et al. (2019) Supporting self-management for people with hypertension: A meta-review of quantitative and qualitative systematic reviews. J Hypertens 37: 264-279. https://doi.org/10.1097/HJH.0000000000001867
|
| [28] |
Du L, Cheng Z, Zhang Y, et al. (2017) The impact of medication adherence on clinical outcomes of coronary artery disease: A meta-analysis. Eur J Prev Cardiolog 24: 962-970. https://doi.org/10.1177/2047487317695628
|
| [29] |
Laranjo L, Lanas F, Sun MC, et al. (2024) World heart federation roadmap for secondary prevention of cardiovascular disease: 2023 Update. Global Heart 19: 8. https://doi.org/10.5334/gh.1278
|
| [30] |
Hamilton SJ, Mills B, Birch EM, et al. (2018) Smartphones in the secondary prevention of cardiovascular disease: A systematic review. BMC Cardiovasc Disord 18: 25. https://doi.org/10.1186/s12872-018-0764-x
|
| [31] |
Xiong S, Berkhouse H, Schooler M, et al. (2018) Effectiveness of mHealth interventions in improving medication adherence among people with hypertension: A systematic review. Curr Hypertens Rep 20: 86. https://doi.org/10.1007/s11906-018-0886-7
|
| [32] |
Gong K, Yan YL, Li Y, et al. (2020) Mobile health applications for the management of primary hypertension: A multicenter, randomized, controlled trial. Medicine (Baltimore) 99: e19715. https://doi.org/10.1097/MD.0000000000019715
|
| [33] |
Persell SD, Peprah YA, Lipiszko D, et al. (2020) Effect of home blood pressure monitoring via a smartphone hypertension coaching application or tracking application on adults with uncontrolled hypertension: A randomized clinical trial. JAMA Netw Open 3: e200255. https://doi.org/10.1001/jamanetworkopen.2020.0255
|
| [34] |
Lippke S, Dahmen A, Gao L, et al. (2021) To what extent is internet activity predictive of psychological well-being?. Psychol Res Behav Manag 14: 207-219. https://doi.org/10.2147/PRBM.S274502
|
| [35] |
Michie S, Richardson M, Johnston M, et al. (2013) The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann Behav Med 46: 81-95. https://doi.org/10.1007/s12160-013-9486-6
|
| [36] |
Audette LM, Hammond MS, Rochester NK (2020) Methodological issues with coding participants in anonymous psychological longitudinal studies. Educ Psychol Meas 80: 163-185. https://doi.org/10.1177/0013164419843576
|
| [37] |
Vargas C, Whelan J, Brimblecombe J, et al. (2022) Co-creation, co-design, co-production for public health–a perspective on definition and distinctions. Public Health Res Pract 32. https://doi.org/10.17061/phrp3222211
|
| [38] |
Schwarzer R, Lippke S, Luszczynska A (2011) Mechanisms of health behavior change in persons with chronic illness or disability: The Health Action Process Approach (HAPA). Rehabil Psychol 56: 161-170. https://doi.org/10.1037/a0024509
|
| [39] |
Connell LE, Carey RN, De Bruin M, et al. (2019) Links between behavior change techniques and mechanisms of action: An expert consensus study. Ann Behav Med 53: 708-720. https://doi.org/10.1093/abm/kay082
|
| [40] |
Fleig L, Lippke S, Pomp S, et al. (2011) Intervention effects of exercise self-regulation on physical exercise and eating fruits and vegetables: A longitudinal study in orthopedic and cardiac rehabilitation. Prev Med 53: 182-187. https://doi.org/10.1016/j.ypmed.2011.06.019
|
| [41] |
Storm V, Dörenkämper J, Reinwand DA, et al. (2016) Effectiveness of a web-based computer-tailored multiple-lifestyle intervention for people interested in reducing their cardiovascular risk: A randomized controlled trial. J Med Internet Res 18: e78. https://doi.org/10.2196/jmir.5147
|
| [42] |
Ganeshan S, Jackson H, Grandis DJ, et al. (2022) Clinical outcomes and qualitative perceptions of in-person, hybrid, and virtual cardiac rehabilitation. J Cardiopulm Rehabil Prev 42: 338-346. https://doi.org/10.1097/HCR.0000000000000688
|
| [43] |
Sangeethalakshmi K, Preethi U, Pavithra S (2023) Patient health monitoring system using IoT. Mater Today Proc 80: 2228-2231. https://doi.org/10.1016/j.matpr.2021.06.188
|
| [44] |
Lippke S, Fleig L, Wiedemann AU, et al. (2015) A computerized lifestyle application to promote multiple health behaviors at the workplace: Testing its behavioral and psychological effects. J Med Internet Res 17: e225. https://doi.org/10.2196/jmir.4486
|
| [45] |
Karhula T, Vuorinen AL, Rääpysjärvi K, et al. (2015) Telemonitoring and mobile phone-based health coaching among Finnish diabetic and heart disease patients: Randomized controlled trial. J Med Internet Res 17: e153. https://doi.org/10.2196/jmir.4059
|
| [46] |
Dickson VV, Lee C, Yehle KS, et al. (2017) Psychometric testing of the self-care of hypertension inventory. J Cardiovasc Nurs 32: 431-438. https://doi.org/10.1097/JCN.0000000000000364
|
| [47] | Norman GR, Sloan JA, Wyrwich KW (2003) Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Med Care 41: 582-592. https://doi.org/10.1097/01.MLR.0000062554.74615.4C |
| [48] |
Riegel B, Lee CS, Dickson VV, et al. (2009) An update on the self-care of heart failure index. J Cardiovasc Nurs 24: 485-497. https://doi.org/10.1097/JCN.0b013e3181b4baa0
|
| [49] |
Craig CL, Marshall AL, Sjöström M, et al. (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35: 1381-1395. https://doi.org/10.1249/01.MSS.0000078924.61453.FB
|
| [50] |
Kambic T, Šarabon N, Hadžić V, et al. (2021) Objectively measured physical activity in patients with coronary artery disease: A cross-validation study. Biosensors (Basel) 11: 318. https://doi.org/10.3390/bios11090318
|
| [51] |
Saran T, Owoc J, Bojar I (2018) Use of the IPAQ questionnaire in the form of a mobile application in monitoring physical activity of patients with cardiovascular diseases. Ann Agric Environ Med 25: 395-402. https://doi.org/10.26444/aaem/75704
|
| [52] |
Stenman E, Leijon ME, Calling S, et al. (2012) Study protocol: A multi-professional team intervention of physical activity referrals in primary care patients with cardiovascular risk factors—the Dalby lifestyle intervention cohort (DALICO) study. BMC Health Serv Res 12: 173. https://doi.org/10.1186/1472-6963-12-173
|
| [53] |
Duschek S, Hoffmann A, Bair A, et al. (2018) Cerebral blood flow modulations during proactive control in chronic hypotension. Brain Cogn 125: 135-141. https://doi.org/10.1016/j.bandc.2018.06.008
|
| [54] |
Bell ML, Whitehead AL, Julious SA (2018) Guidance for using pilot studies to inform the design of intervention trials with continuous outcomes. Clin Epidemiol 10: 153-157. https://doi.org/10.2147/CLEP.S146397
|
| [55] |
Chandler J, Sox L, Kellam K, et al. (2019) Impact of a culturally tailored mhealth medication regimen self-management program upon blood pressure among hypertensive Hispanic adults. Int J Environ Res Public Health 16: 1226. https://doi.org/10.3390/ijerph16071226
|
| [56] |
Guasti L, Dilaveris P, Mamas MA, et al. (2022) Digital health in older adults for the prevention and management of cardiovascular diseases and frailty. A clinical consensus statement from the ESC Council for Cardiology Practice/Taskforce on Geriatric Cardiology, the ESC Digital Health Committee and the ESC Working Group on e-Cardiology. ESC Heart Fail 9: 2808-2822. https://doi.org/10.1002/ehf2.14022
|
| [57] |
Santo K, Singleton A, Rogers K, et al. (2019) Medication reminder applications to improve adherence in coronary heart disease: A randomised clinical trial. Heart 105: 323-329. https://doi.org/10.1136/heartjnl-2018-313479
|
| [58] |
Coorey GM, Neubeck L, Mulley J, et al. (2018) Effectiveness, acceptability and usefulness of mobile applications for cardiovascular disease self-management: Systematic review with meta-synthesis of quantitative and qualitative data. Eur J Prev Cardiol 25: 505-521. https://doi.org/10.1177/2047487317750913
|
| [59] |
Ni YX, Liu XH, He L, et al. (2024) Mobile application-based interventions for people with heart failure: A systematic review and meta-analysis. J Nurs Manage 2024: 6859795. https://doi.org/10.1155/2024/6859795
|
| [60] |
Verloigne M, Altenburg T, Cardon G, et al. (2022) Making co-creation a trustworthy methodology for closing the implementation gap between knowledge and action in health promotion: The Health CASCADE project. Perspect Public Health 143: 196-198. https://doi.org/10.1177/17579139221136718
|
| [61] |
Fleig L, Pomp S, Schwarzer R, et al. (2013) Promoting exercise maintenance: How interventions with booster sessions improve long-term rehabilitation outcomes. Rehabil Psychol 58: 323-333. https://doi.org/10.1037/a0033885
|
| [62] | Adler AJ, Martin N, Mariani J, et al. (2017) Mobile phone text messaging to improve medication adherence in secondary prevention of cardiovascular disease. Cochrane Database Syst Rev 4: CD011851. https://doi.org/10.1002/14651858.CD011851.pub2 |
 publichealth-12-01-015-s001.pdf publichealth-12-01-015-s001.pdf |
 |
Figures(3) / Tables(7)

Sonia Lippke, Luisa Korte, Vinayak Anand Kumar, Andreas Fach, Tiara Ratz. Health behavior and disease self-management indicators in patients with cardiovascular diseases using a health app: Findings from an RCT[J]. AIMS Public Health, 2025, 12(1): 233-258. doi: 10.3934/publichealth.2025015







 DownLoad:
DownLoad: