Vaccines are an essential part of public health interventions to mitigate the devastating health and non-health impacts of COVID-19 pandemic. Despite the fact that Sudan launched the COVID-19 vaccination program in March 2021, only 10% of the population received their two primary doses of vaccines by the end of May 2022. This delayed uptake of vaccines obviously warrants investigation. Therefore, we have conducted this study to evaluate the knowledge, attitude and acceptance of the general population in Sudan toward COVID-19 vaccines.
A descriptive cross-sectional community-based study. The data were collected using an electronic questionnaire from 403 individuals living in Khartoum, Sudan. The data were processed using the Statistical Package for Social Sciences (SPSS), and data analysis was performed using appropriate tests.
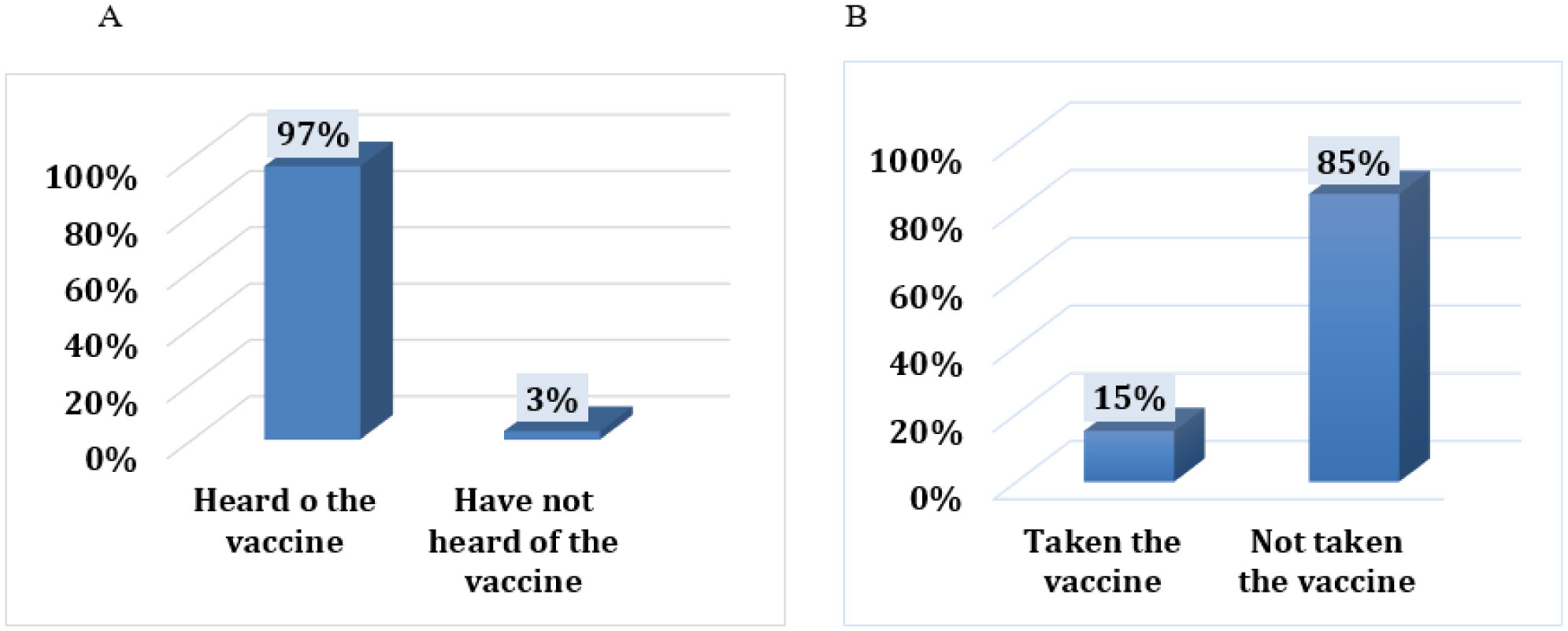
51% of the participants were found to have sufficient knowledge about the COVID-19 vaccine, and the knowledge level is higher among those educated beyond the secondary school and those who were employed. Among those unvaccinated, only 47% of the participants expressed their intention to take the vaccine when offered to them. The major reason for not trusting the vaccine is safety concerns expressed by 65.5% of the unvaccinated.
Higher education levels and employment were associated with an increase in sufficient knowledge about the vaccine in around half of the participants. However, most of participants had not taken the vaccine at the time of the study, and the trust in vaccines is not high. Effective interventions by the health authorities are needed to address these issues in order to accelerate the COVID-19 vaccination program in Sudan.
Citation: Safaa Badi, Loai Abdelgadir Babiker, Abdullah Yasseen Aldow, Almigdad Badr Aldeen Abas, Mazen Abdelhafiez Eisa, Mohamed Nour Abu-Ali, Wagass Abdelrhman Abdella, Mohamed Elsir Marzouq, Musaab Ahmed, Abubakr Ali M Omer, Mohamed H Ahmed. Knowledge and attitudes toward COVID-19 vaccination in Sudan: A cross-sectional study[J]. AIMS Public Health, 2023, 10(2): 310-323. doi: 10.3934/publichealth.2023023
Vaccines are an essential part of public health interventions to mitigate the devastating health and non-health impacts of COVID-19 pandemic. Despite the fact that Sudan launched the COVID-19 vaccination program in March 2021, only 10% of the population received their two primary doses of vaccines by the end of May 2022. This delayed uptake of vaccines obviously warrants investigation. Therefore, we have conducted this study to evaluate the knowledge, attitude and acceptance of the general population in Sudan toward COVID-19 vaccines.
A descriptive cross-sectional community-based study. The data were collected using an electronic questionnaire from 403 individuals living in Khartoum, Sudan. The data were processed using the Statistical Package for Social Sciences (SPSS), and data analysis was performed using appropriate tests.
51% of the participants were found to have sufficient knowledge about the COVID-19 vaccine, and the knowledge level is higher among those educated beyond the secondary school and those who were employed. Among those unvaccinated, only 47% of the participants expressed their intention to take the vaccine when offered to them. The major reason for not trusting the vaccine is safety concerns expressed by 65.5% of the unvaccinated.
Higher education levels and employment were associated with an increase in sufficient knowledge about the vaccine in around half of the participants. However, most of participants had not taken the vaccine at the time of the study, and the trust in vaccines is not high. Effective interventions by the health authorities are needed to address these issues in order to accelerate the COVID-19 vaccination program in Sudan.

| [1] |
Jiang F, Deng L, Zhang L, et al. (2019) Review of the Clinical Characteristics of Coronavirus Disease. J Gen Intern Med 35: 1545-1549. https://doi.org/10.1007/s11606-020-05762-w 
|
| [2] |
Zhao J, Zhao S, Ou J, et al. (2020) COVID-19: coronavirus vaccine development updates. Front Immunol 11: 602256. https://doi.org/10.3389/fimmu.2020.602256
|
| [3] |
Ura T, Yamashita A, Mizuki N, et al. (2020) New vaccine production platforms used in developing SARS-CoV-2 vaccine candidates. Vaccine 39: 197-201. https://doi.org/10.1016/j.vaccine.2020.11.054
|
| [4] |
Fang E, Liu X, Li M, et al. (2022) Advances in COVID-19 mRNA vaccine development. Signal Transduct Target Ther 7: 94. https://doi.org/10.1038/s41392-022-00950-y
|
| [5] |
Xia S, Duan K, Zhang Y, et al. (2020) Effect of an inactivated vaccine against SARS-CoV-2 on safety and immunogenicity outcomes: interim analysis of 2 randomized clinical trials. JAMA 324: 951-960. https://doi.org/10.1001/jama.2020.15543
|
| [6] | Jadaan SA, Khan AW (2022) Recent update of COVID-19 vaccines. Adv Pharm Bull 12: 219-236. https://doi.org/10.34172/apb.2022.045 |
| [7] |
Anyanwu JC, Salami AO (2021) The impact of COVID-19 on African economies: An introduction. Afr Dev Rev 33: S1-S16. https://doi.org/10.1111/1467-8268.12531
|
| [8] | Samal C, Jakimowicz K, Dasgupta K, et al. (2021) Vaccination Worldwide: Strategies, Distribution and Challenges. arXiv . 2107.14139 |
| [9] |
Leach M, MacGregor H, Akello G, et al. (2022) Vaccine anxieties, vaccine preparedness: perspectives from Africa in a Covid-19 era. Soc Sci Med 298: 114826. https://doi.org/10.1016/j.socscimed.2022.114826
|
| [10] | Owid/covid-19-data. Available from: https://github.com/owid/covid-19-data/blob/master/public/data/vaccinations/locations.csv. |
| [11] |
Dubé E, Laberge C, Guay M, et al. (2013) Vaccine hesitancy: an overview. Hum Vaccin Immunother 9: 1763-1773. https://doi.org/10.4161/hv.24657
|
| [12] |
Garett R, Young SD (2021) Online misinformation and vaccine hesitancy. Transl Behav Med 11: 2194-2199. https://doi.org/10.1093/tbm/ibab128
|
| [13] |
Karakose T, Ozdemir TY, Papadakis S, et al. (2022) Investigating the relationships between COVID-19 quality of life, loneliness, happiness, and internet addiction among K-12 teachers and school administrators—a structural equation modeling approach. Int J Environ Res Public Health 19: 1052. https://doi.org/10.3390/ijerph19031052
|
| [14] |
Karakose T, Yirci R, Papadakis S (2022) Examining the associations between COVID-19-related psychological distress, social media addiction, COVID-19-related burnout, and depression among school principals and teachers through structural equation modeling. Int J Environ Res Public Health 19: 1951. https://doi.org/10.3390/ijerph19041951
|
| [15] |
Karakose T, Yirci R, Papadakis S (2021) Exploring the interrelationship between covid-19 phobia, work–family conflict, family–work conflict, and life satisfaction among school administrators for advancing sustainable management. Sustainability 13: 8654. https://doi.org/10.3390/su13158654
|
| [16] |
Mahmud S, Mohsin M, Khan IA, et al. (2021) Knowledge, beliefs, attitudes and perceived risk about COVID-19 vaccine and determinants of COVID-19 vaccine acceptance in Bangladesh. PLoS One 16: e0257096. https://doi.org/10.1371/journal.pone.0257096
|
| [17] |
Abebe H, Shitu S, Mose A (2021) Understanding of COVID-19 vaccine knowledge, attitude, acceptance, and determinates of COVID-19 vaccine acceptance among adult population in Ethiopia. Infect Drug Resist 14: 2015-2025. https://doi.org/10.2147/IDR.S312116
|
| [18] |
Fakonti G, Kyprianidou M, Toumbis G, et al. (2021) Knowledge and attitudes toward vaccination among nurses and midwives in Cyprus: A cross-sectional study. Int J Nurs Knowl 33: 321-329. https://doi.org/10.1111/2047-3095.12354
|
| [19] |
Alabdulla M, Reagu S M, Al-Khal A, et al. (2021) COVID-19 vaccine hesitancy and attitudes in Qatar: A national cross-sectional survey of a migrant-majority population. Influenza Other Respir Viruses 15: 361-370. https://doi.org/10.1111/irv.12847
|
| [20] |
Akalu Y, Ayelign B, Molla MD (2020) Knowledge, attitude and practice towards covid-19 among chronic disease patients at addis zemen hospital, Northwest Ethiopia. Infect Drug Resist 13: 1949-1960. https://doi.org/10.2147/IDR.S258736
|
| [21] | Mudenda S, Mukosha M, Meyer JC, et al. (2021) Awareness and Acceptance of COVID-19 Vaccines among Pharmacy Students in Zambia: The Implications for Addressing Vaccine Hesitancy. Research Square : 1-22. https://doi.org/10.21203/rs.3.rs-651501/v1 |
| [22] | Sallam M, Dababseh D, Eid H, et al. (2021) High rates of COVID-19 vaccine hesitancy and its association with conspiracy beliefs: a study in Jordan and Kuwait among other Arab countries. Vaccines 9: 1-16. https://doi.org/10.3390/vaccines9010042 |
| [23] |
Al-Qerem WA, Jarab AS (2021) COVID-19 vaccination acceptance and its associated factors among a Middle Eastern population. Front Public Health 9: 632914. https://doi.org/10.3389/fpubh.2021.632914
|
| [24] |
El-Elimat T, AbuAlSamen MM, Almomani BA, et al. (2021) Acceptance and attitudes toward COVID-19 vaccines: A cross-sectional study from Jordan. PLoS One 16: e0250555. https://doi.org/10.1371/journal.pone.0250555
|
| [25] |
Al-Mohaithef M, Padhi BK (2020) Determinants of COVID-19 vaccine acceptance in Saudi Arabia: a web-based national survey. J Multidiscip Healthc 13: 1657-1663. https://doi.org/10.2147/JMDH.S276771
|
| [26] |
Faezi NA, Gholizadeh P, Sanogo M, et al. (2021) Peoples' attitude toward COVID-19 vaccine, acceptance, and social trust among African and Middle East countries. Health Promot Perspect 11: 171-178. https://doi.org/10.34172/hpp.2021.21
|
| [27] |
Syed Alwi SAR, Rafidah E, Zurraini A, et al. (2021) A survey on COVID-19 vaccine acceptance and concern among Malaysians. BMC Public Health 21: 1129. https://doi.org/10.1186/s12889-021-11071-6
|
| [28] |
Bai W, Cai H, Liu S, et al. (2021) Attitudes toward COVID-19 vaccines in Chinese college students. Int J Biol Sci 17: 1469-1475. https://doi.org/10.7150/ijbs.58835
|
| [29] |
Makki S, Siddiqua A, Wahab S, et al. (2022) Beliefs and Barriers to COVID-19 Vaccine Acceptance in Three Countries with Different Human Development Index (HDI) Scores: A Comparative Study. Patient Prefer Adherence 16: 3257-3265. https://doi.org/10.2147/PPA.S393956
|
| [30] |
Elbadawi MH, Altayib LS, Birier ABG, et al. (2022) Beliefs and barriers of COVID-19 vaccination hesitancy among Sudanese healthcare workers in Sudan: A cross sectional study. Hum Vaccin Immunother 18: 2132082. https://doi.org/10.1080/21645515.2022.2132082
|
| [31] | Yassin EOM, Faroug HAA, Ishaq ZBY, et al. (2022) COVID-19 vaccination acceptance among healthcare staff in Sudan, 2021. J Immunol Res 2022: 3392667. https://doi.org/10.1155/2022/3392667 |
| [32] |
Raja SM, Osman ME, Musa AO, et al. (2022) COVID-19 vaccine acceptance, hesitancy, and associated factors among medical students in Sudan. PLoS One 17: e0266670. https://doi.org/10.1371/journal.pone.0266670
|
| [33] |
Omar SM, Khalil R, Adam I, et al. (2022) The Concern of COVID-19 Vaccine Safety Is behind Its Low Uptake among Patients with Diabetes Mellitus in Sudan. Vaccines 10: 527. https://doi.org/10.3390/vaccines10040527
|
| [34] |
Elbarazi I, Yacoub M, Reyad OA, et al. (2022) Exploring enablers and barriers toward COVID-19 vaccine acceptance among Arabs: A qualitative study. Int J Disaster Risk Reduct 82: 103304. https://doi.org/10.1016/j.ijdrr.2022.103304
|
| [35] |
Coccia M (2023) Effects of strict containment policies on COVID-19 pandemic crisis: lessons to cope with next pandemic impacts. Environ Sci Pollut Res Int 30: 2020-2028. https://doi.org/10.1007/s11356-022-22024-w
|
| [36] |
Coccia M (2022) Optimal levels of vaccination to reduce COVID-19 infected individuals and deaths: A global analysis. Environ Res 204: 112314. https://doi.org/10.1016/j.envres.2021.112314
|
| [37] |
Coccia M (2022) Improving preparedness for next pandemics: Max level of COVID-19 vaccinations without social impositions to design effective health policy and avoid flawed democracies. Environ Res 213: 113566. https://doi.org/10.1016/j.envres.2022.113566
|
| [38] |
Coccia M (2022) COVID-19 pandemic over 2020 (with lockdowns) and 2021 (with vaccinations): similar effects for seasonality and environmental factors. Environ Res 208: 112711. https://doi.org/10.1016/j.envres.2022.112711
|
| [39] |
Coccia M (2022) Preparedness of countries to face COVID-19 pandemic crisis: Strategic positioning and factors supporting effective strategies of prevention of pandemic threats. Environ Res 203: 111678. https://doi.org/10.1016/j.envres.2021.111678
|
Figures(3) / Tables(4)

Safaa Badi, Loai Abdelgadir Babiker, Abdullah Yasseen Aldow, Almigdad Badr Aldeen Abas, Mazen Abdelhafiez Eisa, Mohamed Nour Abu-Ali, Wagass Abdelrhman Abdella, Mohamed Elsir Marzouq, Musaab Ahmed, Abubakr Ali M Omer, Mohamed H Ahmed. Knowledge and attitudes toward COVID-19 vaccination in Sudan: A cross-sectional study[J]. AIMS Public Health, 2023, 10(2): 310-323. doi: 10.3934/publichealth.2023023







 DownLoad:
DownLoad: