Neck and back pain afflicts millions of people. Magnetotherapy has shown to have anti-inflammatory effects that could act on pain generation, but the literature lacks provide a precise therapeutic protocol.
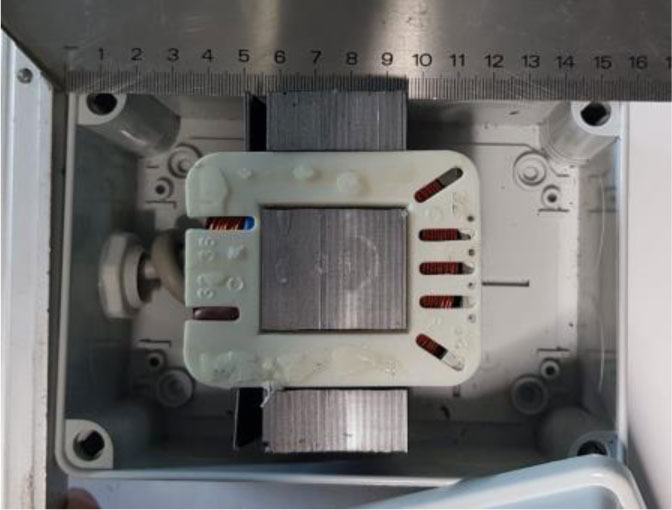
A high-intensity electromagnetic field with a dedicated applicator was administered to 38 patients with low-back pain and 30 patients with neck pain. The device provides 60 mT and a frequency of 50 Hz for 30 minutes, the session was repeated 4 times.
The mean VAS of the low-back pain group decreased from 6.56 to 4.54, with a significant reduction of 30.8%. The mean VAS of the neck pain group decreased from 6.51 to 1.96, with a significant reduction of 69.9%.
The treatment used showed good results in both groups of the patient, without side effects. The therapeutic protocol adopted is safe, provide rapid relief from the pain and is not time demanding. This treatment could represent an effective non-pharmacologic physical therapy option in the treatment of low-back pain and cervical pain.
Citation: Mattia Fortina, Aurelio Vittoria, Stefano Giannotti, Pasquale Biandolino, Gabriele Cevenini, Serafino Carta. Short time effects of a low-frequency, high intensity magnetic field in the treatment of chronic neck and low back pain[J]. AIMS Public Health, 2022, 9(2): 307-315. doi: 10.3934/publichealth.2022021
Neck and back pain afflicts millions of people. Magnetotherapy has shown to have anti-inflammatory effects that could act on pain generation, but the literature lacks provide a precise therapeutic protocol.
A high-intensity electromagnetic field with a dedicated applicator was administered to 38 patients with low-back pain and 30 patients with neck pain. The device provides 60 mT and a frequency of 50 Hz for 30 minutes, the session was repeated 4 times.
The mean VAS of the low-back pain group decreased from 6.56 to 4.54, with a significant reduction of 30.8%. The mean VAS of the neck pain group decreased from 6.51 to 1.96, with a significant reduction of 69.9%.
The treatment used showed good results in both groups of the patient, without side effects. The therapeutic protocol adopted is safe, provide rapid relief from the pain and is not time demanding. This treatment could represent an effective non-pharmacologic physical therapy option in the treatment of low-back pain and cervical pain.

| [1] | Manek NJ, McGregor AJ (2005) Epidemiology of back disorders: prevalence, risk factors, and prognosis. Curr Opin Rheumatolo 17: 134-140. https://doi.org/10.1097/01.bor.0000154215.08986.06 |
| [2] |
Shahidi B, Curran-Everett D, Maluf KS (2015) Psychosocial, physical, and neurophysiological risk factors for chronic neck pain: a prospective inception cohort study. J Pain 16: 1288-1299. https://doi.org/10.1016/j.jpain.2015.09.002 
|
| [3] |
Sihawong R, Sitthipornvorakul E, Paksaichol A, et al. (2016) Predictors for chronic neck and low back pain in office workers: a 1-year prospective cohort study. J Occup Health 58: 16-24. https://doi.org/10.1539/joh.15-0168-OA
|
| [4] |
Hoy D, Bain C, Williams G, et al. (2012) A systematic review of the global prevalence of low back pain. Arthritis Rheum 64: 2028-2037. https://doi.org/10.1002/art.34347
|
| [5] |
Garcia AN, Costa LC, da Silva TM, et al. (2013) Effectiveness of back school versus McKenzie exercises in patients with chronic nonspecific low back pain: a randomized controlled trial. Phys Ther 93: 729-747. https://doi.org/10.2522/ptj.20120414
|
| [6] |
Van Tulder M, Koes B, Bombardier C (2002) Low back pain. Best Pract Res Clin Rheumatol 16: 761-775. https://doi.org/10.1053/berh.2002.0267
|
| [7] |
Gerdesmeyer L, Wagenpfeil S, Birkenmaier C, et al. (2013) Percutaneous epidural lysis of adhesions in chronic lumbar radicular pain: a randomized, double-blind, placebo-controlled trial. Pain Physician 16: 185-196. https://doi.org/10.36076/ppj.2013/16/185
|
| [8] | Rubik B (1997) Bioelectromagnetics and the future of medicine. Adm Radiol J 16: 38-46. |
| [9] |
Vincenzi F, Targa M, Corciulo C, et al. (2013) Pulsed electromagnetic fields increased the anti-inflammatory effect of A(2)A and A(3) adenosine receptors in human T/C-28a2 chondrocytes and hFOB 1.19 osteoblasts. Plos One 8: e65561. https://doi.org/10.1371/journal.pone.0065561
|
| [10] |
Albanese A, Battisti E, Pompella G, et al. (2009) Preliminary studies about effects of ELF and TAMMEF electromagnetic fields on human lymphomonocytes. Environmentalist 29: 196-199. https://doi.org/10.1007/s10669-008-9207-z
|
| [11] | Battisti E, Piazza E, Rigato M, et al. (2004) Efficacy and safety of a musically modulated field (TAMMEF) in patients affected by knee osteoarthitis. Clin Exp Rheumatol 22: 568-572. |
| [12] |
Battisti E, Albanese A, Bianciardi L, et al. (2009) Tammef therapy in the treatment of shoulder periarthritis: efficacy and safety. Environmentalist 29: 190-195. https://doi.org/10.1007/s10669-008-9202-4
|
| [13] |
Rigato M, Battisti E, Fortunato M, et al. (2002) Comparison between the analgesic and therapeutic effects of a musically modulated electromagnetic field (TAMMEF) and those of a 100Hz electromagnetic field: blind experiment on patients suffering from cervical spondylosis or shoulder periarthritis. J Med Eng Technol 26: 253-258. https://doi.org/10.1080/0309190021000025873
|
| [14] |
Battisti E, Albanese A, Bianciardi L, et al. (2007) Efficacy and safety of new TAMMEF (therapeutic application of musically modulated electromagnetic fields) system in the treatment of chronic low back pain. Environmentalist 27: 441-445. https://doi.org/10.1007/s10669-007-9081-0
|
| [15] | Kroeling P, Gross A, Graham N, et al. (2013) Electrotherapy for neck pain. Cochrane Database Syst Rev 8: CD004251. https://doi.org/10.1002/14651858.CD004251.pub4 |
| [16] |
Andrade R, Duarte H, Pereira R, et al. (2006) Pulsed electromagnetic field therapy effectiveness in low back pain: A systematic review of randomized controlled trials. Porto Biomed J 1: 156-163. https://doi.org/10.1016/j.pbj.2016.09.001
|
| [17] |
Fardon DF, Williams AL, Dohring EJ, et al. (2014) Lumbar disc nomenclature: version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine J 14: 2525-2545. https://doi.org/10.1016/j.spinee.2014.04.022
|
| [18] |
Van Rijn JC, Klemetso N, Reitsma JB, et al. (2005) Observer variation in MRI evaluation of patients suspected of lumbar disk herniation. AJR Am J Roentgenol 184: 299-303. https://doi.org/10.2214/ajr.184.1.01840299
|
| [19] | Giordano N, Battisti E, Geraci S, et al. (2000) Analgesic-antiinflammatory effect of 100 Hz variable magnetic field in R.A.. Clin Exp Rheumatol 18: 263. |
| [20] |
Giordano N, Battisti E, Geraci S, et al. (2001) Effect of electromagnetic fields on bone density and biochemical markers of bone turnover in osteoporosis: a single blind, randomized pilot study. Curr Ther Res Clin Exp 62: 187-193. https://doi.org/10.1016/S0011-393X(01)80030-8
|
| [21] |
Li JK, Lin JC, Liu HC, et al. (2007) Cytokine release from osteoblasts in response to different intensities of pulsed electromagnetic field stimulation. Electromagn Biol Med 26: 153-165. https://doi.org/10.1080/15368370701572837
|
| [22] |
Paungmali A, Henry LJ, Sitilertpisan P, et al. (2006) Improvements in tissue blood flow and lumbopelvic stability after lumbopelvic core stabilization training in patients with chronic non-specific low back pain. J Phys Ther Sci 28: 635-640. https://doi.org/10.1589/jpts.28.635
|

Figures(2) / Tables(2)

Mattia Fortina, Aurelio Vittoria, Stefano Giannotti, Pasquale Biandolino, Gabriele Cevenini, Serafino Carta. Short time effects of a low-frequency, high intensity magnetic field in the treatment of chronic neck and low back pain[J]. AIMS Public Health, 2022, 9(2): 307-315. doi: 10.3934/publichealth.2022021







 DownLoad:
DownLoad: