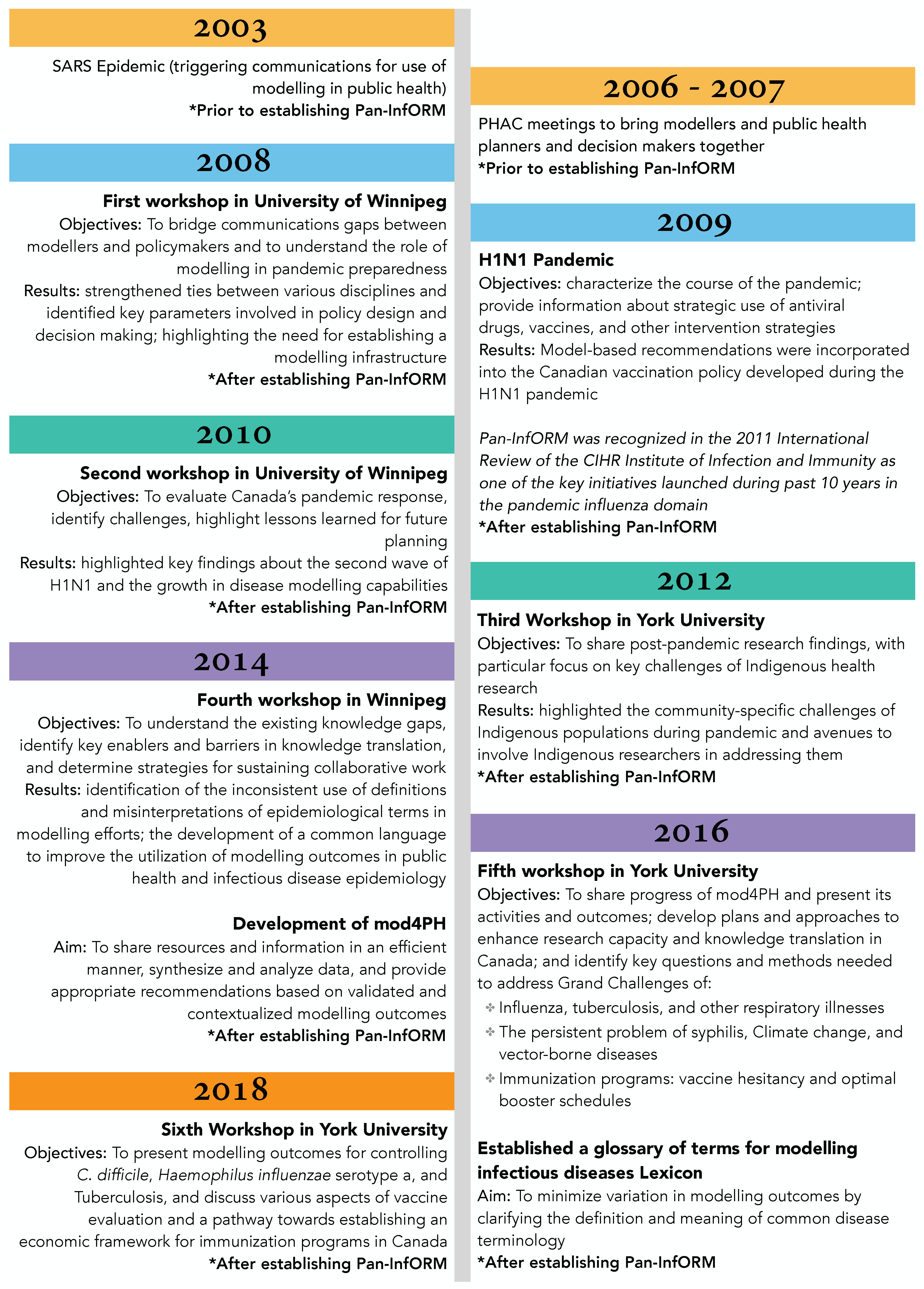
Modelling and simulation methods can play an important role in guiding public health responses to infectious diseases and emerging health threats by projecting the plausible outcomes of decisions and interventions. The 2003 SARS epidemic marked a new chapter in disease modelling in Canada as it triggered a national discussion on the utility and uptake of modelling research in local and pandemic outbreaks. However, integration and application of model-based outcomes in public health requires knowledge translation and contextualization. We reviewed the history and performance of Pan-InfORM (Pandemic Influenza Outbreak Research Modelling), which created a national infrastructure in Canada with a mandate to develop innovative knowledge translation methodologies to inform policy makers through modelling frameworks that bridge the gaps between theory, policy, and practice. This review demonstrates the importance of a collaborative infrastructure as a “Community of Practice” to guide public health responses, especially in the context of emerging diseases with substantial uncertainty, such as the COVID-19 pandemic. Dedicated resources to modelling and knowledge translation activities can help create synergistic strategies at the global scale and optimize public health responses to protect at-risk populations and quell socioeconomic and health burden.
Citation: Mehreen Tariq, Margaret Haworth-Brockman, Seyed M Moghadas. Ten years of Pan-InfORM: modelling research for public health in Canada[J]. AIMS Public Health, 2021, 8(2): 265-274. doi: 10.3934/publichealth.2021020
Modelling and simulation methods can play an important role in guiding public health responses to infectious diseases and emerging health threats by projecting the plausible outcomes of decisions and interventions. The 2003 SARS epidemic marked a new chapter in disease modelling in Canada as it triggered a national discussion on the utility and uptake of modelling research in local and pandemic outbreaks. However, integration and application of model-based outcomes in public health requires knowledge translation and contextualization. We reviewed the history and performance of Pan-InfORM (Pandemic Influenza Outbreak Research Modelling), which created a national infrastructure in Canada with a mandate to develop innovative knowledge translation methodologies to inform policy makers through modelling frameworks that bridge the gaps between theory, policy, and practice. This review demonstrates the importance of a collaborative infrastructure as a “Community of Practice” to guide public health responses, especially in the context of emerging diseases with substantial uncertainty, such as the COVID-19 pandemic. Dedicated resources to modelling and knowledge translation activities can help create synergistic strategies at the global scale and optimize public health responses to protect at-risk populations and quell socioeconomic and health burden.

| [1] | Pan-InfORM Pan-InfORM: Pandemic Influenza Outbreak Research Modelling Available from: http://pan-inform.yorku.ca/. |
| [2] |
Lathlean J, May AL (2002) Communities of practice: an opportunity for interagency working. J Clin Nurs 11: 394-398. doi: 10.1046/j.1365-2702.2002.00630.x

|
| [3] | Wenger E, McDermott RA, Snyder W (2002) Cultivating Communities of Practice: A Guide to Managing Knowledge Harvard Business Press. |
| [4] |
Chowell G, Castillo-Chavez C, Fenimore PW, et al. (2004) Model Parameters and Outbreak Control for SARS. Emerg Infect Dis 10: 1258-1263. doi: 10.3201/eid1007.030647
|
| [5] |
Moghadas SM, Pizzi NJ, Wu J, et al. (2009) Managing public health crises: the role of models in pandemic preparedness. Influenza Other Respir Viruses 3: 75-79. doi: 10.1111/j.1750-2659.2009.00081.x
|
| [6] | Pan-InfORM (2009) Modelling an influenza pandemic: A guide for the perplexed. CMAJ Can Med Assoc J 181: 171-173. |
| [7] | Star L, Moghadas SM The Role of Mathematical Modelling in Public Health Planning and Decision Making. National Collaborating Centre for Infectious Diseases (2015) .Available from: https://nccid.ca/publications/the-role-of-mathematical-modelling-in-public-health-planning-and-decision-making/. |
| [8] | Canadian Institutes of Health Research Internal Assessment for 2011 International Review - CIHR Institute of Infection and Immunity - CIHR (2011) .Available from: https://cihr-irsc.gc.ca/e/43717.html. |
| [9] |
Moghadas SM, Pizzi NJ, Wu J, et al. (2011) Canada in the face of the 2009 H1N1 pandemic. Influenza Other Respir Viruses 5: 83-88. doi: 10.1111/j.1750-2659.2010.00184.x
|
| [10] | Mostaço-Guidolin L, Pizzi N, Moghadas S (2011) A classical approach for estimating the transmissibility of the 2009 H1N1 pandemic. Can Appl Math Q 19. |
| [11] |
Mostaço-Guidolin LC, Greer A, Sander B, et al. (2011) Variability in transmissibility of the 2009 H1N1 pandemic in Canadian communities. BMC Res Notes 4: 537. doi: 10.1186/1756-0500-4-537
|
| [12] |
Bowman CS, Arino J, Moghadas SM (2011) Evaluation of vaccination strategies during pandemic outbreaks. Math Biosci Eng MBE 8: 113-122. doi: 10.3934/mbe.2011.8.113
|
| [13] |
Laskowski M, Mostaço-Guidolin LC, Greer AL, et al. (2011) The Impact of Demographic Variables on Disease Spread: Influenza in Remote Communities. Sci Rep 1: 105. doi: 10.1038/srep00105
|
| [14] |
Richardson KL, Driedger MS, Pizzi NJ, et al. (2012) Indigenous populations health protection: A Canadian perspective. BMC Public Health 12: 1098. doi: 10.1186/1471-2458-12-1098
|
| [15] | Moghadas SM Optimal Treatment Strategies for Remote and Isolated Communities. National Collaborating Centre for Infectious Diseases (2015) .Available from: https://nccid.ca/publications/optimal-treatment-strategies-for-remote-and-isolated-communities/. |
| [16] |
Driedger S, Cooper EJ, Moghadas SM (2014) Developing model-based public health policy through knowledge translation: The need for a ‘Communities of Practice’. Public Health 128. doi: 10.1016/j.puhe.2013.10.009
|
| [17] |
Moghadas SM, Haworth-Brockman M, Isfeld-Kiely H, et al. (2015) Improving public health policy through infection transmission modelling: Guidelines for creating a Community of Practice. Can J Infect Dis Med Microbiol 26: 191-195. doi: 10.1155/2015/274569
|
| [18] | Laskowski M, Moghadas SM Review of Terms Used in Modelling Influenza Infection. National Collaborating Centre for Infectious Diseases (2015) .Available from: https://nccid.ca/publications/review-of-terms-used-in-modelling-influenza-infection/. |
| [19] | NCCID mod4PH – Modelling for Public Health. National Collaborating Centre for Infectious Diseases (2020) .Available from: https://www.linkedin.com/groups/6787233/. |
| [20] |
Milwid R, Steriu A, Arino J, et al. (2016) Toward Standardizing a Lexicon of Infectious Disease Modeling Terms. Front Public Health 4. doi: 10.3389/fpubh.2016.00213
|
| [21] | Pan-InfORM, NCCID, ICID Public Health Challenges for Modelling and Infectious Diseases From “Communities of Practice” to “Communities of Health”, Public Health Workshop (2016) .Available from: http://pan-inform.yorku.ca/events/pan-inform-workshop-2016.html. |
| [22] | World Health Organization WHO End TB Strategy, Global strategy and targets for tuberculosis prevention, care and control after 2015 (2013) .Available from: http://www.who.int/tb/post2015_strategy/en/. |
| [23] | Halseth R, Odulaja OO (2018) Addressing the challenge of latent tuberculosis infection among Indigenous peoples in Canada. Natl Collab Cent Aborig Health 40. |
| [24] | NCCID, NCCEH Canadian Databases for Disease Vectors. National Collaborating Centre for Infectious Diseases (2018) .Available from: https://nccid.ca/publications/canadian-databases-disease-vectors/. |
| [25] | National Collaborating Centre for Infectious Diseases Mathematical Modelling in Public Health (2018) .Available from: https://nccid.ca/webcast/iq14-behind-the-curtain-of-mathematical-modelling/. |
| [26] | Pan-InfORM, NCCID (2018) Modelling Outcomes and Knowledge Translation: From Research to Policy and Practice. |
| [27] | National Collaborating Centre for Infectious Diseases Mathematical Modelling in Public Health Planning: Flu Vaccine (2020) .Available from: https://nccid.ca/publications/mathematical-modelling-in-public-health-planning-flu-vaccine/. |
| [28] | National Collaborating Centre for Infectious Diseases Mathematical Modelling in Public Health: Tuberculosis (2020) .Available from: https://nccid.ca/publications/mathematical-modelling-in-public-health-tuberculosis/. |
Figures(1)

Mehreen Tariq, Margaret Haworth-Brockman, Seyed M Moghadas. Ten years of Pan-InfORM: modelling research for public health in Canada[J]. AIMS Public Health, 2021, 8(2): 265-274. doi: 10.3934/publichealth.2021020







 DownLoad:
DownLoad: