Attention deficit hyperactivity disorder (ADHD) manifests itself in inattention, impulsivity, and/or hyperactivity. Those affected with ADHD have high motor coordination or motor performance problems, which presents as a daily difficulty. On the other hand, physical activity can produce motor benefits and ADHD symptomatology. Therefore, the aim of this systematic review is to analyze the effects of physical activity, sport, exercise, play or physical education interventions on the motor performance of children and adolescents with ADHD (registry: INPLASY202370105). The databases PubMed (87), Scopus (133), WoS (126), and SciELO (0) were searched using the keywords “Children” OR “Adolescent” AND “ADHD” OR “attention-deficit/hyperactivity disorder” OR “attention deficit hyperactivity disorder” AND “Motor skills” OR “Motor coordination” OR “Motor Performance” OR “Motor impairment” AND “Physical activity” OR “Exercise” OR “Sports” OR “Physical Education” OR “Play” OR “Pretend play”. 14 studies met the inclusion criteria. The PEDro scale and risk of bias were used to evaluate the methodological quality of the selected articles. Benefits were evidenced in motor skills, cognitive functions, executive functions, and academic and social performance in children and adolescents with ADHD.
Citation: Nathacha Garcés, Angel Jara, Felipe Montalva-Valenzuela, Claudio Farías-Valenzuela, Gerson Ferrari, Paloma Ferrero-Hernández, Antonio Castillo-Paredes. Motor performance in children and adolescents with attention deficit and hyperactivity disorder: A systematic review[J]. AIMS Medical Science, 2025, 12(2): 247-267. doi: 10.3934/medsci.2025017
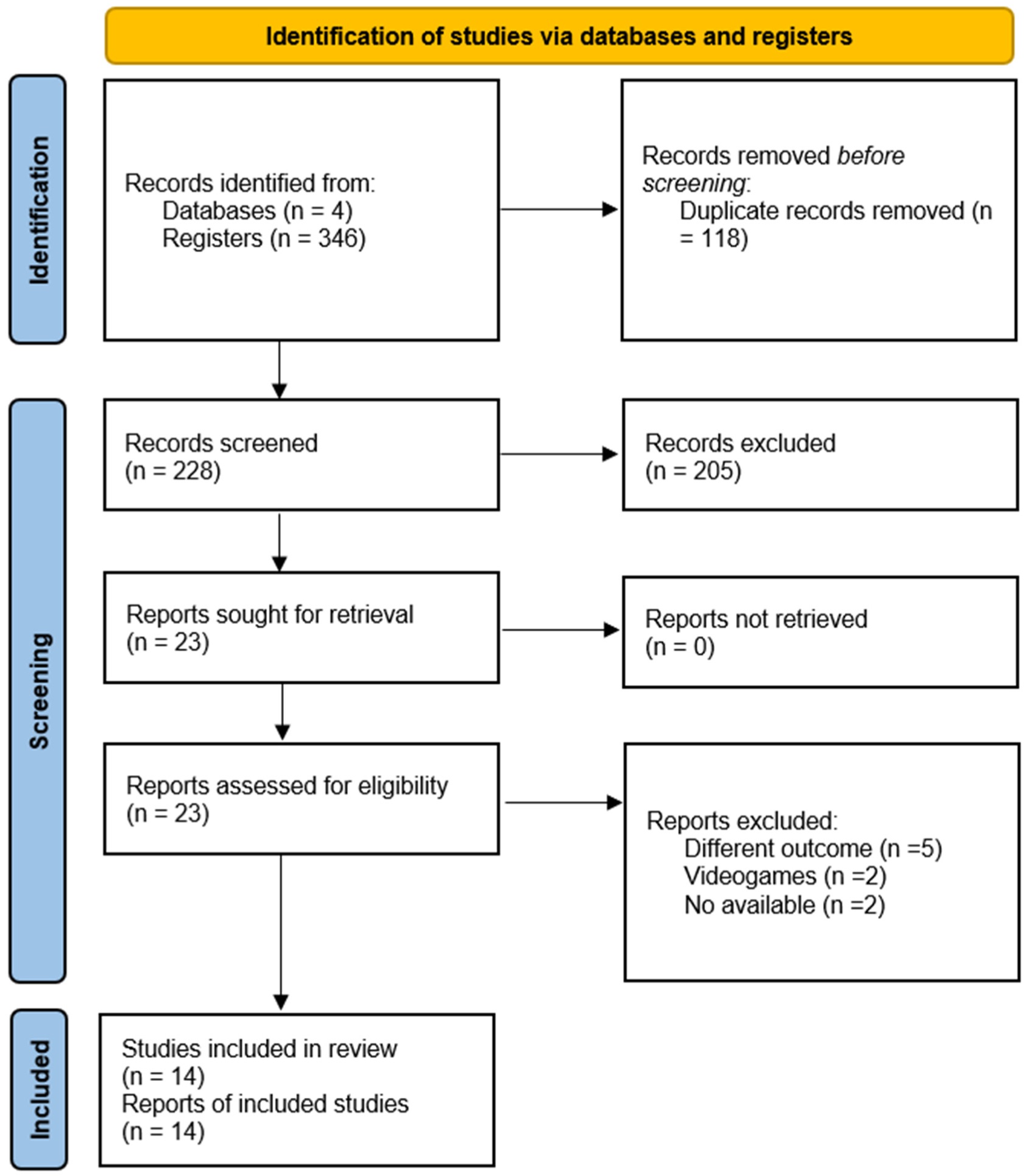
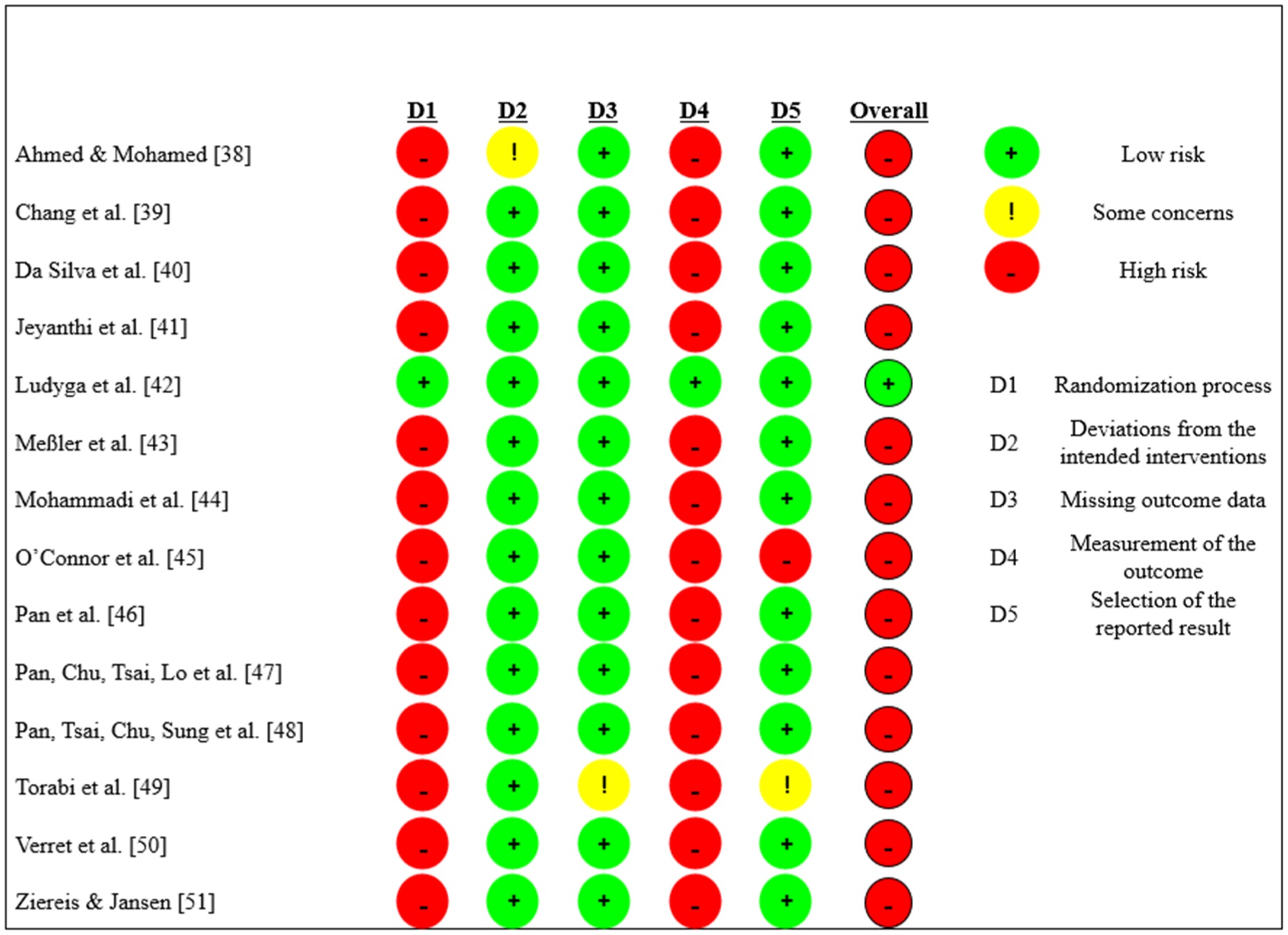
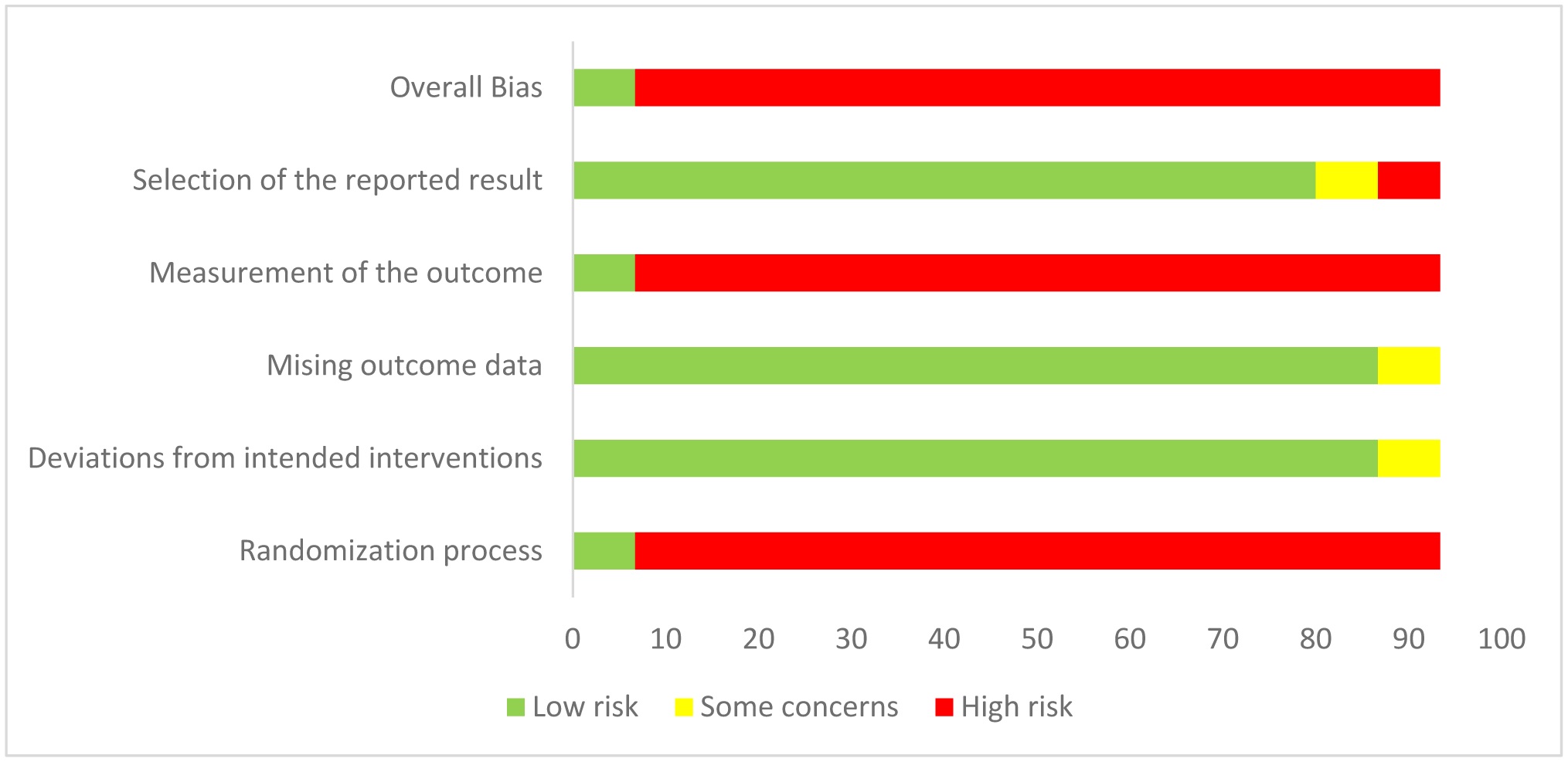
Attention deficit hyperactivity disorder (ADHD) manifests itself in inattention, impulsivity, and/or hyperactivity. Those affected with ADHD have high motor coordination or motor performance problems, which presents as a daily difficulty. On the other hand, physical activity can produce motor benefits and ADHD symptomatology. Therefore, the aim of this systematic review is to analyze the effects of physical activity, sport, exercise, play or physical education interventions on the motor performance of children and adolescents with ADHD (registry: INPLASY202370105). The databases PubMed (87), Scopus (133), WoS (126), and SciELO (0) were searched using the keywords “Children” OR “Adolescent” AND “ADHD” OR “attention-deficit/hyperactivity disorder” OR “attention deficit hyperactivity disorder” AND “Motor skills” OR “Motor coordination” OR “Motor Performance” OR “Motor impairment” AND “Physical activity” OR “Exercise” OR “Sports” OR “Physical Education” OR “Play” OR “Pretend play”. 14 studies met the inclusion criteria. The PEDro scale and risk of bias were used to evaluate the methodological quality of the selected articles. Benefits were evidenced in motor skills, cognitive functions, executive functions, and academic and social performance in children and adolescents with ADHD.

| [1] | (2013) American Psychiatric AssociationTrastornos del Neurodesarrollo (5ª. ed). Manual Diagnóstico y Estadístico de los Trastornos Mentales . España: Médica Panamericana 32. |
| [2] |
Alderson RM, Rapport MD, Kofler M (2007) Attention-deficit/hyperactivity disorder and behavioral inhibition: A meta-analytic review of the stop-signal paradigm. J Abnorm Child Psychol 35: 745-758. https://doi.org/10.1007/s10802-007-9131-6 
|
| [3] |
Noordermeer SDS, Luman M, Buitelaar JK, et al. (2020) Neurocognitive deficits in attention-deficit/hyperactivity disorder with and without comorbid oppositional defiant disorder. J Atten Disord 24: 1317-1329. https://doi.org/10.1177/1087054715606216
|
| [4] |
Faraone SV, Banaschewski T, Coghill D, et al. (2021) The world federation of ADHD international consensus statement: 208 evidence-based conclusions about the disorder. Neurosci Biobehav Rev 128: 789-818. https://doi.org/10.1016/j.neubiorev.2021.01.022
|
| [5] |
Gallego-Méndez J, Perez-Gomez J, Calzada-Rodríguez JI, et al. (2020) Relationship between health-related quality of life and physical activity in children with hyperactivity. Int J Environ Res Public Health 17: 2804. https://doi.org/10.3390/ijerph17082804
|
| [6] |
LeFever GB, Villers MS, Morrow AL, et al. (2002) Parental perceptions of adverse educational outcomes among children diagnosed and treated for ADHD: A call for improved school/provider collaboration. Psychol Schools 39: 63-71. https://doi.org/10.1002/pits.10000
|
| [7] |
Weibel S, Menard O, Ionita A, et al. (2020) Practical considerations for the evaluation and management of Attention Deficit Hyperactivity Disorder (ADHD) in adults. L'Encephale 46: 30-40. https://doi.org/10.1016/j.encep.2019.06.005
|
| [8] |
Sharma A, Couture J (2014) A review of the pathophysiology, etiology, and treatment of attention-deficit hyperactivity disorder (ADHD). Ann Pharmacother 48: 209-225. https://doi.org/10.1177/1060028013510699
|
| [9] |
Dahan A, Ryder CH, Reiner M (2018) Components of motor deficiencies in ADHD and possible interventions. Neuroscience 378: 34-53. https://doi.org/10.1016/j.neuroscience.2016.05.040
|
| [10] |
Kaiser ML, Schoemaker MM, Albaret JM, et al. (2015) What is the evidence of impaired motor skills and motor control among children with attention deficit hyperactivity disorder (ADHD)? Systematic review of the literature. Res Dev Disabil 36: 338-357. https://doi.org/10.1016/j.ridd.2014.09.023
|
| [11] |
Meachon EJ, Klupp S, Grob A (2023) Gait in children with and without ADHD: A systematic literature review. Gait Posture 104: 31-42. https://doi.org/10.1016/j.gaitpost.2023.06.003
|
| [12] | Mokobane M, Pillay BJ, Meyer A (2019) Fine motor deficits and attention deficit hyperactivity disorder in primary school children. S Afr J Psychi 25: 1232. https://doi.org/10.4102/sajpsychiatry.v25i0.1232 |
| [13] |
Villa de Gregorio M, Ruiz Pérez LM, Barriopedro Moro MI (2019) Analysis of the relationships between low motor competence and attention and hyperactivity problems in school age. Retos 36: 625-632. https://doi.org/10.47197/retos.v36i36.68502
|
| [14] |
Fliers E, Rommelse N, Vermeulen SHHM, et al. (2008) Motor coordination problems in children and adolescents with ADHD rated by parents and teachers: effects of age and gender. J Neural Transm 115: 211-220. https://doi.org/10.1007/s00702-007-0827-0
|
| [15] |
Polanczyk G, de Lima MS, Horta BL, et al. (2007) The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiat 164: 942-948. https://doi.org/10.1176/ajp.2007.164.6.942
|
| [16] |
Skinner RA, Piek JP (2001) Psychosocial implications of poor motor coordination in children and adolescents. Hum Mov Sci 20: 73-94. https://doi.org/10.1016/S0167-9457(01)00029-X
|
| [17] |
Skalidou S, Anestis A, Bakolas N, et al. (2023) Swimming activity alleviates the symptoms of Attention Deficit Hyperactivity Disorder (ADHD) a case report. Healthcare 11: 1999. https://doi.org/10.3390/healthcare1114199
|
| [18] |
Villa M, Barriopedro Moro MI, Ruiz Pérez LM (2020) Motor competence difficulties and attention deficit and hyperactivity disorder (ADHD) among secondary students. Cuadernos de Psicología del Deporte 20: 47-62. https://doi.org/10.6018/cpd.360491
|
| [19] | Carriedo A (2014) B enefits of physical education in children diagnosedwith attention deficit hyperactivity disorder (ADHD). J Sport Health Res 6: 60. |
| [20] |
Rezende LFM, Garcia LMT, Mielke GI, et al. (2019) Physical activity and preventable premature deaths from non-communicable diseases in Brazil. J Public Health 41: e253-e260. https://doi.org/10.1093/pubmed/fdy183
|
| [21] |
Martín-Martínez I, Chirosa LJ, Reigal RE, et al. (2015) Effects of physical activity on executive function in a sample of adolescents. Anales de Psicología 31: 962. https://doi.org/10.6018/analesps.31.3.171601
|
| [22] | Romero López M, Benavides Nieto A, Fernández Cabezas M, et al. (2017) Intervention in executive functions in early childhood education. Int J Dev Educ Psychol 3: 253-261. https://doi.org/10.17060/ijodaep.2017.n1.v3.994 |
| [23] |
Villalta Páucar MA, Budnik CA, Valencia SM (2013) Conocimiento escolar y procesos cognitivos en la interacción didáctica en la sala de clase. Perfiles Educativos 35: 84-96. https://doi.org/10.1016/S0185-2698(13)71836-1
|
| [24] |
Reloba S, Chirosa LJ, Reigal RE (2016) Relation of physical activity, cognitive and academic performance in children: Review of current literature. Revista Andaluza de Medicina Del Deporte 9: 166-172. https://doi.org/10.1016/j.ramd.2015.05.008
|
| [25] |
Gualdi-Russo E, Zaccagni L (2021) Physical activity for health and wellness. Int J Environ Res Public Health 18: 7823. https://doi.org/10.3390/ijerph18157823
|
| [26] |
Fisher A, Boyle JM, Paton JY, et al. (2011) Effects of a physical education intervention on cognitive function in young children: randomized controlled pilot study. BMC Pediatr 11: 97. https://doi.org/10.1186/1471-2431-11-97
|
| [27] |
Silva Piñeiro R, Mayán Santos JM (2016) Psychological benefits of a proactive physical exercise program for elderly people. Escritos de Psicología (Internet) 9: 24-32. https://doi.org/10.24310/espsiescpsi.v9i1.13197
|
| [28] |
Snedden TR, Scerpella J, Kliethermes SA, et al. (2019) Sport and physical activity level impacts health-related quality of life among collegiate students. Am J Health Promot 33: 675-682. https://doi.org/10.1177/0890117118817715
|
| [29] |
Palma Marifil T, Carroza Sepulveda D, Torres Lorca R, et al. (2021) Changes in the symptoms of inattention, hyperactivity and impulsivity in children and adolescents with ADHD through Sports. A review. Retos 41: 701-707. https://doi.org/10.47197/retos.v41i0.78201
|
| [30] | Montalva-Valenzuela F, Andrades-Ramírez O, Castillo-Paredes A (2022) Effects of physical activity, exercise and sport on executive function in young people with attention deficit hyperactivity disorder: a systematic review. Eur J Invest Health Psychol Educ 12: 61-76. https://doi.org/10.3390/ejihpe12010006 |
| [31] |
Müller P, Duderstadt Y, Lessmann V, et al. (2020) Lactate and BDNF: key mediators of exercise induced neuroplasticity?. J Clin Med 9: 1136. https://doi.org/10.3390/jcm9041136
|
| [32] |
Page MJ, McKenzie JE, Bossuyt PM, et al. (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol 74: 790-799. https://doi.org/10.1016/j.recesp.2021.06.016
|
| [33] |
Santos CM da C, Pimenta CA de M, Nobre MRC (2007) The PICO strategy for the research question construction and evidence search. Rev Latino-Am Enfermagem 15: 508-511. https://doi.org/10.1590/S0104-11692007000300023
|
| [34] |
Martínez Díaz JD, Ortega Chacón V, Muñoz Ronda FJ (2016) Design of clinical questions in evidence-based practice. Formulation models. Enferm Glob 15: 431-438.
|
| [35] | Cascaes SF, Valdivia ABA, da Rosa IR, et al. (2013) Evaluation lists and scales for the quality of scientific studies. Rev Cuba Inf Cienc Salud 24: 295-312. |
| [36] |
De Morton NA (2009) The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother 55: 129-133. https://doi.org/10.1016/S0004-9514(09)70043-1
|
| [37] |
Herbert R, Moseley A, Sherrington C, et al. (2000) Physiotherapy evidence database. Physiotherapy 86: 55. https://doi.org/10.1016/S0031-9406(05)61357-0
|
| [38] | Ahmed G, Mohamed S (2011) Effect of regular aerobic exercises on behavioral, cognitive and psychological response in patients with attention deficit-hyperactivity disorder. Life Sci J 8: 366-371. http://www.dx.doi.org/10.7537/marslsj080211.50 |
| [39] |
Chang YK, Hung CL, Huang CJ, et al. (2014) Effects of an aquatic exercise program on inhibitory control in children with ADHD: a preliminary study. Arch Clin Neuropsychol 29: 217-223. https://doi.org/10.1093/arclin/acu003
|
| [40] |
Da Silva LA, Doyenart R, Henrique Salvan P, et al. (2020) Swimming training improves mental health parameters, cognition and motor coordination in children with Attention Deficit Hyperactivity Disorder. Int J Environ Health Res 30: 584-592. https://doi.org/10.1080/09603123.2019.1612041
|
| [41] |
Jeyanthi S, Arumugam N, Parasher RK (2021) Effectiveness of structured exercises on motor skills, physical fitness and attention in children with ADHD compared to typically developing children-A pilot study. ENeurologicalSci 24: 100357. https://doi.org/10.1016/j.ensci.2021.100357
|
| [42] |
Ludyga S, Mücke M, Leuenberger R, et al. (2022) Behavioral and neurocognitive effects of judo training on working memory capacity in children with ADHD: A randomized controlled trial. NeuroImage-Clin 36: 103156. https://doi.org/10.1016/j.nicl.2022.103156
|
| [43] |
Meßler CF, Holmberg HC, Sperlich B (2018) Multimodal therapy involving high-intensity interval training improves the physical fitness, motor skills, social behavior, and quality of life of boys with ADHD: a randomized controlled study. J Atten Disord 22: 806-812. https://doi.org/10.1177/1087054716636936
|
| [44] | Mohammadi Orangi B, Yaali R, Ghorbanzadeh B, et al. (2021) The effect of aerobic exercise with nonlinear pedagogy on anxiety, depression, motor proficiency and cognitive ability of boys with Attention Deficit Hyperactivity Disorder. J Rehabil Sci Res 8: 144-150. https://doi.org/10.30476/jrsr.2021.91068.1163 |
| [45] |
O'Connor BC, Fabiano GA, Waschbusch DA, et al. (2014) Effects of a summer treatment program on functional sports outcomes in young children with ADHD. J Abnorm Child Psychol 42: 1005-1017. https://doi.org/10.1007/s10802-013-9830-0
|
| [46] |
Pan CY, Chang YK, Tsai CL, et al. (2017) Effects of physical activity intervention on motor proficiency and physical fitness in children with ADHD: an exploratory study. J Atten Disord 21: 783-795. https://doi.org/10.1177/1087054714533192
|
| [47] |
Pan CY, Chu CH, Tsai CL, et al. (2016) A racket-sport intervention improves behavioral and cognitive performance in children with attention-deficit/hyperactivity disorder. Res Dev Disabil 57: 1-10. https://doi.org/10.1016/j.ridd.2016.06.009
|
| [48] |
Pan CY, Tsai CL, Chu CH, et al. (2019) Effects of physical exercise intervention on motor skills and executive functions in children with ADHD: a pilot study. J Atten Disord 23: 384-397. https://doi.org/10.1177/1087054715569282
|
| [49] |
Torabi F, Farahani A, Safakish S, et al. (2018) Evaluation of motor proficiency and adiponectin in adolescent students with attention deficit hyperactivity disorder after high-intensity intermittent training. Psychiatry Res 261: 40-44. https://doi.org/10.1016/j.psychres.2017.12.053
|
| [50] |
Verret C, Guay MC, Berthiaume C, et al. (2012) A physical activity program improves behavior and cognitive functions in children with ADHD. J Atten Disord 16: 71-80. https://doi.org/10.1177/1087054710379735
|
| [51] |
Ziereis S, Jansen P (2015) Effects of physical activity on executive function and motor performance in children with ADHD. Res Dev Disabil 38: 181-191. https://doi.org/10.1016/j.ridd.2014.12.005
|
| [52] |
Jørgensen L, Paludan-Müller AS, Laursen DR, et al. (2016) Evaluation of the Cochrane tool for assessing risk of bias in randomized clinical trials: overview of published comments and analysis of user practice in Cochrane and non-Cochrane reviews. Syst Rev 5: 80. https://doi.org/10.1186/s13643-016-0259-8
|
| [53] |
Han A, Fu A, Cobley S, et al. (2018) Effectiveness of exercise intervention on improving fundamental movement skills and motor coordination in overweight/obese children and adolescents: A systematic review. J Sci Med Sport 21: 89-102. https://doi.org/10.1016/j.jsams.2017.07.001
|
| [54] |
Bünger A, Urfer-Maurer N, Grob A (2021) Multimethod assessment of attention, executive functions, and motor skills in children with and without ADHD: children's performance and parents' perceptions. J Atten Disord 25: 596-606. https://doi.org/10.1177/1087054718824985
|
| [55] |
Barnard-Brak L, Davis T, Sulak T, et al. (2011) The association between physical education and symptoms of Attention Deficit Hyperactivity Disorder. J Phys Act Health 8: 964-970. https://doi.org/10.1123/jpah.8.7.964
|
| [56] | Rivera AL, Remón ÁLC (2017) Benefits of physical and sporting activity for children with ADHD. EmásF: revista digital de educación física 44: 63-78. |
| [57] |
Mehren A, Özyurt J, Lam AP, et al. (2019) Acute effects of aerobic exercise on executive function and attention in adult patients With ADHD. Front Psychiatry 10: 132. https://doi.org/10.3389/fpsyt.2019.00132
|
| [58] | Rodríguez Torres ÁF, Rodríguez Alvear JC, Guerrero Gallardo HI, et al. (2020) Physical activity benefits for children and adolescents in the school. Rev Cubana Med Gen Integr 36: e1535. |
Figures(3) / Tables(2)

Nathacha Garcés, Angel Jara, Felipe Montalva-Valenzuela, Claudio Farías-Valenzuela, Gerson Ferrari, Paloma Ferrero-Hernández, Antonio Castillo-Paredes. Motor performance in children and adolescents with attention deficit and hyperactivity disorder: A systematic review[J]. AIMS Medical Science, 2025, 12(2): 247-267. doi: 10.3934/medsci.2025017







 DownLoad:
DownLoad: