Calcified coronary lesions pose significant challenges in percutaneous coronary intervention, which can impede device placement and stent expansion, thus leading to suboptimal clinical outcomes. This paper outlines a comprehensive approach for the safe and effective preparation of calcified lesions. It emphasizes the importance of pre-procedural planning using either coronary artery calcium scoring or computed tomography coronary angiography, as well as advanced intravascular imaging techniques with intravascular ultrasound and optical coherence tomography for accurate lesion assessment. Various lesion modification strategies are reviewed, including balloon angioplasty, rotational atherectomy, orbital atherectomy, laser atherectomy, and lithotripsy. The selection criteria for each technique based on the lesion characteristics, calcium morphology, and operator experience are discussed. Additionally, clinical data is analysed to provide evidence-based recommendations for practice. The paper concludes with a discussion on future directions and innovations alongside a proposed algorithm for the management of calcified coronary lesions, which is aimed at improving patient outcomes through technological advancements and refined procedural techniques.
Citation: Bharat Khialani, Sara Malakouti, Sandeep Basavarajah, Leontin Lazar, Sylwia Iwanczyk, Bernardo Cortese. How to identify and prepare calcified lesions safely and effectively[J]. AIMS Medical Science, 2025, 12(2): 171-192. doi: 10.3934/medsci.2025011
Calcified coronary lesions pose significant challenges in percutaneous coronary intervention, which can impede device placement and stent expansion, thus leading to suboptimal clinical outcomes. This paper outlines a comprehensive approach for the safe and effective preparation of calcified lesions. It emphasizes the importance of pre-procedural planning using either coronary artery calcium scoring or computed tomography coronary angiography, as well as advanced intravascular imaging techniques with intravascular ultrasound and optical coherence tomography for accurate lesion assessment. Various lesion modification strategies are reviewed, including balloon angioplasty, rotational atherectomy, orbital atherectomy, laser atherectomy, and lithotripsy. The selection criteria for each technique based on the lesion characteristics, calcium morphology, and operator experience are discussed. Additionally, clinical data is analysed to provide evidence-based recommendations for practice. The paper concludes with a discussion on future directions and innovations alongside a proposed algorithm for the management of calcified coronary lesions, which is aimed at improving patient outcomes through technological advancements and refined procedural techniques.

| [1] |
Guedeney P, Claessen BE, Mehran R, et al. (2020) Coronary calcification and long-term outcomes according to drug-eluting stent generation. JACC Cardiovasc Interv 13: 1417-1428. https://doi.org/10.1016/j.jcin.2020.03.053 
|
| [2] | Redfors B, Maehara A, Witzenbichler B, et al. (2017) Outcomes after successful percutaneous coronary intervention of calcified lesions using rotational atherectomy, cutting-balloon angioplasty, or balloon-only angioplasty before drug-eluting stent implantation. J Invasive Cardiol 29: 378-386. |
| [3] |
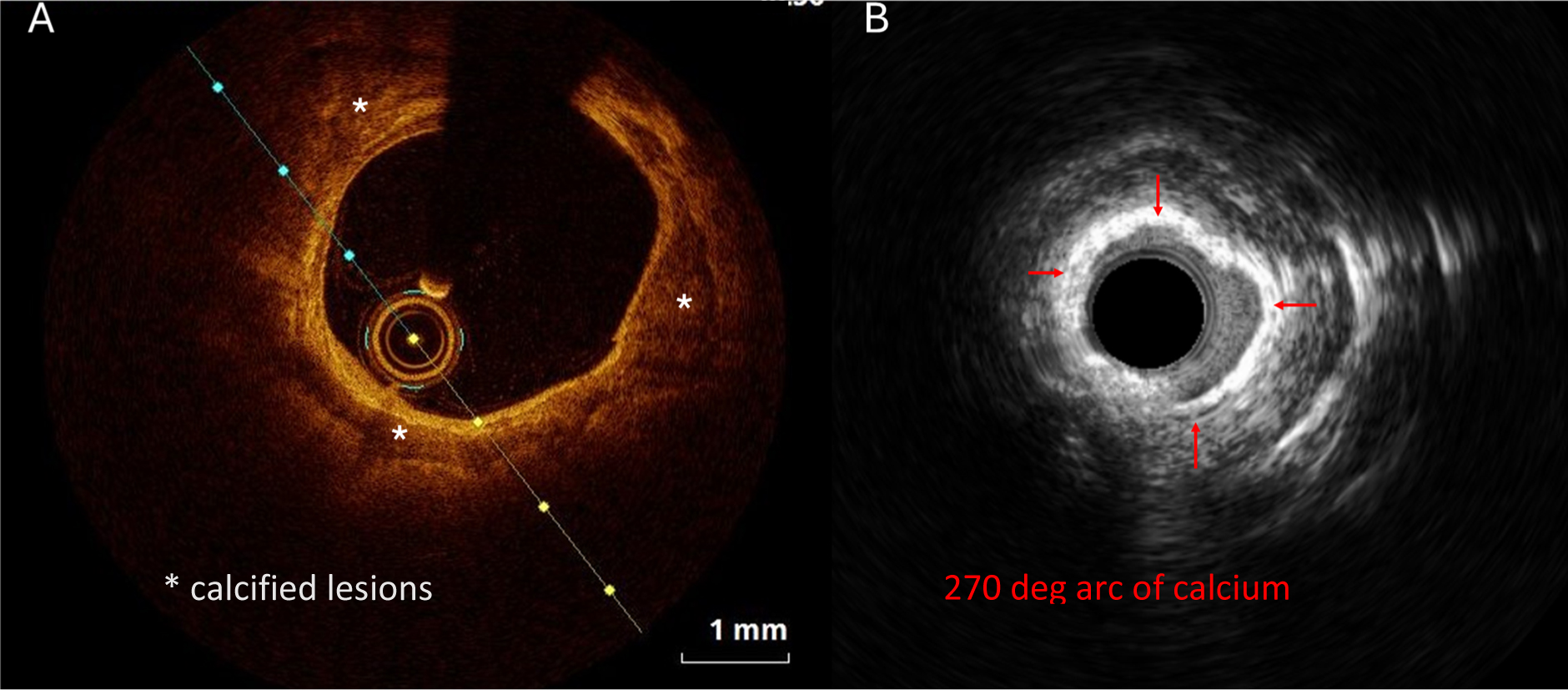
Wang X, Matsumura M, Mintz GS, et al. (2017) In vivo calcium detection by comparing optical coherence tomography, intravascular ultrasound, and angiography. JACC Cardiovasc Imaging 10: 869-879. https://doi.org/10.1016/j.jcmg.2017.05.014
|
| [4] |
Mintz GS (2015) Intravascular imaging of coronary calcification and its clinical implications. JACC Cardiovasc Imaging 8: 461-471. https://doi.org/10.1016/j.jcmg.2015.02.003
|
| [5] |
Shah M, Najam O, Bhindi R, et al. (2021) Calcium modification techniques in complex percutaneous coronary intervention. Circ Cardiovasc Interv 14: e009870. https://doi.org/10.1161/CIRCINTERVENTIONS.120.009870
|
| [6] |
De Maria GL, Scarsini R, Banning AP (2019) Management of calcific coronary artery lesions: Is it time to change our interventional therapeutic approach?. JACC Cardiovasc Interv 12: 1465-1478. https://doi.org/10.1016/j.jcin.2019.03.038
|
| [7] |
Jurado-Román A, Gómez-Menchero A, Rivero-Santana B, et al. (2025) Rotational atherectomy, lithotripsy, or laser for calcified coronary stenosis: the ROLLER COASTR-EPIC22 trial. JACC Cardiovasc Interv 18: 606-618. https://doi.org/10.1016/j.jcin.2024.11.012
|
| [8] |
Mintz GS, Popma JJ, Pichard AD, et al. (1995) Patterns of calcification in coronary artery disease. Circulation 91: 1959-1965. https://doi.org/10.1161/01.CIR.91.7.1959
|
| [9] |
Polonsky TS, McClelland RL, Jorgensen NW, et al. (2010) Coronary artery calcium score and risk classification for coronary heart disease prediction. JAMA 303: 1610-1616. https://doi.org/10.1001/jama.2010.461
|
| [10] |
Miller JM, Rochitte CE, Dewey M, et al. (2008) Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med 359: 2324-2336. https://doi.org/10.1056/NEJMoa0806576
|
| [11] |
Budoff MJ, Dowe D, Jollis JG, et al. (2008) Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 52: 1724-1732. https://doi.org/10.1016/j.jacc.2008.07.031
|
| [12] |
Abbara S, Arbab-Zadeh A, Callister TQ, et al. (2009) SCCT guidelines for performance of coronary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 3: 190-204. https://doi.org/10.1016/j.jcct.2009.03.004
|
| [13] |
Araki M, Park SJ, Dauerman HL, et al. (2022) Optical coherence tomography in coronary atherosclerosis assessment and intervention. Nat Rev Cardiol 19: 684-703. https://doi.org/10.1038/s41569-022-00687-9
|
| [14] |
Kawai K, Sato Y, Hokama JY, et al. (2023) Histology, OCT, and micro-CT evaluation of coronary calcification treated with intravascular lithotripsy: atherosclerotic cadaver study. JACC Cardiovasc Interv 16: 2097-2108. https://doi.org/10.1016/j.jcin.2023.06.021
|
| [15] |
Gruslova AB, Singh S, Hoyt T, et al. (2024) Accuracy of OCT core labs in identifying vulnerable plaque. JACC Cardiovasc Imaging 17: 448-450. https://doi.org/10.1016/j.jcmg.2023.10.005
|
| [16] |
de Graaf MA, Broersen A, Kitslaar PH, et al. (2013) Automatic quantification and characterization of coronary atherosclerosis with computed tomography coronary angiography: cross-correlation with intravascular ultrasound virtual histology. Int J Cardiovasc Imaging 29: 1177-1190. https://doi.org/10.1007/s10554-013-0194-x
|
| [17] |
Kim SY, Kim KS, Seung MJ, et al. (2010) The culprit lesion score on multi-detector computed tomography can detect vulnerable coronary artery plaque. Int J Cardiovasc Imaging 26: 245-252. https://doi.org/10.1007/s10554-010-9712-2
|
| [18] |
Mintz GS, Nissen SE, Anderson WD, et al. (2001) American College of Cardiology clinical expert consensus document on standards for acquisition, measurement and reporting of intravascular ultrasound studies (ivus)33. J Am Coll Cardiol 37: 1478-1492. https://doi.org/10.1016/S0735-1097(01)01175-5
|
| [19] |
Zhang M, Matsumura M, Usui E, et al. (2021) Intravascular ultrasound-derived calcium score to predict stent expansion in severely calcified lesions. Circ Cardiovasc Interv 14: e010296. https://doi.org/10.1161/CIRCINTERVENTIONS.120.010296
|
| [20] |
Pu J, Mintz GS, Biro S, et al. (2014) Insights into echo-attenuated plaques, echolucent plaques, and plaques with spotty calcification: novel findings from comparisons among intravascular ultrasound, near-infrared spectroscopy, and pathological histology in 2,294 human coronary artery segments. J Am Coll Cardiol 63: 2220-2233. https://doi.org/10.1016/j.jacc.2014.02.576
|
| [21] |
Mehanna E, Bezerra HG, Prabhu D, et al. (2013) Volumetric characterization of human coronary calcification by frequency-domain optical coherence tomography. Circ J 77: 2334-2340. https://doi.org/10.1253/circj.cj-12-1458
|
| [22] |
Maehara A, Mintz GS, Stone GW (2013) OCT versus IVUS: accuracy versus clinical utility. JACC Cardiovasc Imaging 6: 1105-1107. https://doi.org/10.1016/j.jcmg.2013.05.016
|
| [23] |
Fujino A, Mintz GS, Matsumura M, et al. (2018) A new optical coherence tomography-based calcium scoring system to predict stent underexpansion. EuroIntervention 13: e2182-e2189. https://doi.org/10.4244/EIJ-D-17-00962
|
| [24] |
Généreux P, Madhavan MV, Mintz GS, et al. (2014) Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) TRIALS. J Am Coll Cardiol 63: 1845-1854. https://doi.org/10.1016/j.jacc.2014.01.034
|
| [25] |
Bourantas CV, Zhang YJ, Garg S, et al. (2014) Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention: a patient-level pooled analysis of 7 contemporary stent trials. Heart 100: 1158-1164. https://doi.org/10.1136/heartjnl-2013-305180
|
| [26] |
Silvain J, Lattuca B, Beygui F, et al. (2020) Ticagrelor versus clopidogrel in elective percutaneous coronary intervention (ALPHEUS): a randomised, open-label, phase 3b trial. Lancet 396: 1737-1744. https://doi.org/10.1016/S0140-6736(20)32236-4
|
| [27] |
Alfonso F, Macaya C, Goicolea J, et al. (1994) Determinants of coronary compliance in patients with coronary artery disease: an intravascular ultrasound study. J Am Coll Cardiol 23: 879-884. https://doi.org/10.1016/0735-1097(94)90632-7
|
| [28] |
Madhavan MV, Tarigopula M, Mintz GS, et al. (2014) Coronary artery calcification: pathogenesis and prognostic implications. J Am Coll Cardiol 63: 1703-1714. https://doi.org/10.1016/j.jacc.2014.01.017
|
| [29] |
Huisman J, van der Heijden LC, Kok MM, et al. (2017) Two-year outcome after treatment of severely calcified lesions with newer-generation drug-eluting stents in acute coronary syndromes: a patient-level pooled analysis from TWENTE and DUTCH PEERS. J Cardiol 69: 660-665. https://doi.org/10.1016/j.jjcc.2016.06.010
|
| [30] |
Généreux P, Redfors B, Witzenbichler B, et al. (2017) Angiographic predictors of 2-year stent thrombosis in patients receiving drug-eluting stents: insights from the ADAPT-DES study. Catheter Cardiovasc Interv 89: 26-35. https://doi.org/10.1002/ccd.26409
|
| [31] | Kitahara H, Kobayashi Y, Yamaguchi M, et al. (2008) Damage to polymer of undelivered sirolimus-eluting stents. J Invasive Cardiol 20: 130-133. |
| [32] |
Lee JB, Mintz GS, Lisauskas JB, et al. (2011) Histopathologic validation of the intravascular ultrasound diagnosis of calcified coronary artery nodules. Am J Cardiol 108: 1547-1551. https://doi.org/10.1016/j.amjcard.2011.07.014
|
| [33] |
Watanabe H, Morimoto T, Natsuaki M, et al. (2022) Comparison of clopidogrel monotherapy after 1 to 2 months of dual antiplatelet therapy with 12 months of dual antiplatelet therapy in patients with acute coronary syndrome: the STOPDAPT-2 ACS randomized clinical trial. JAMA Cardiol 7: 407-417. https://doi.org/10.1001/jamacardio.2021.5244
|
| [34] |
Jaspattananon A, Wongpraparut N, Chotinaiwattarakul C, et al. (2021) A risk predictive model for coronary perforation in patients undergoing percutaneous coronary intervention—APOLLO-XI score. European Heart Journal 42: ehab724.2151. https://doi.org/10.1093/eurheartj/ehab724.2151
|
| [35] |
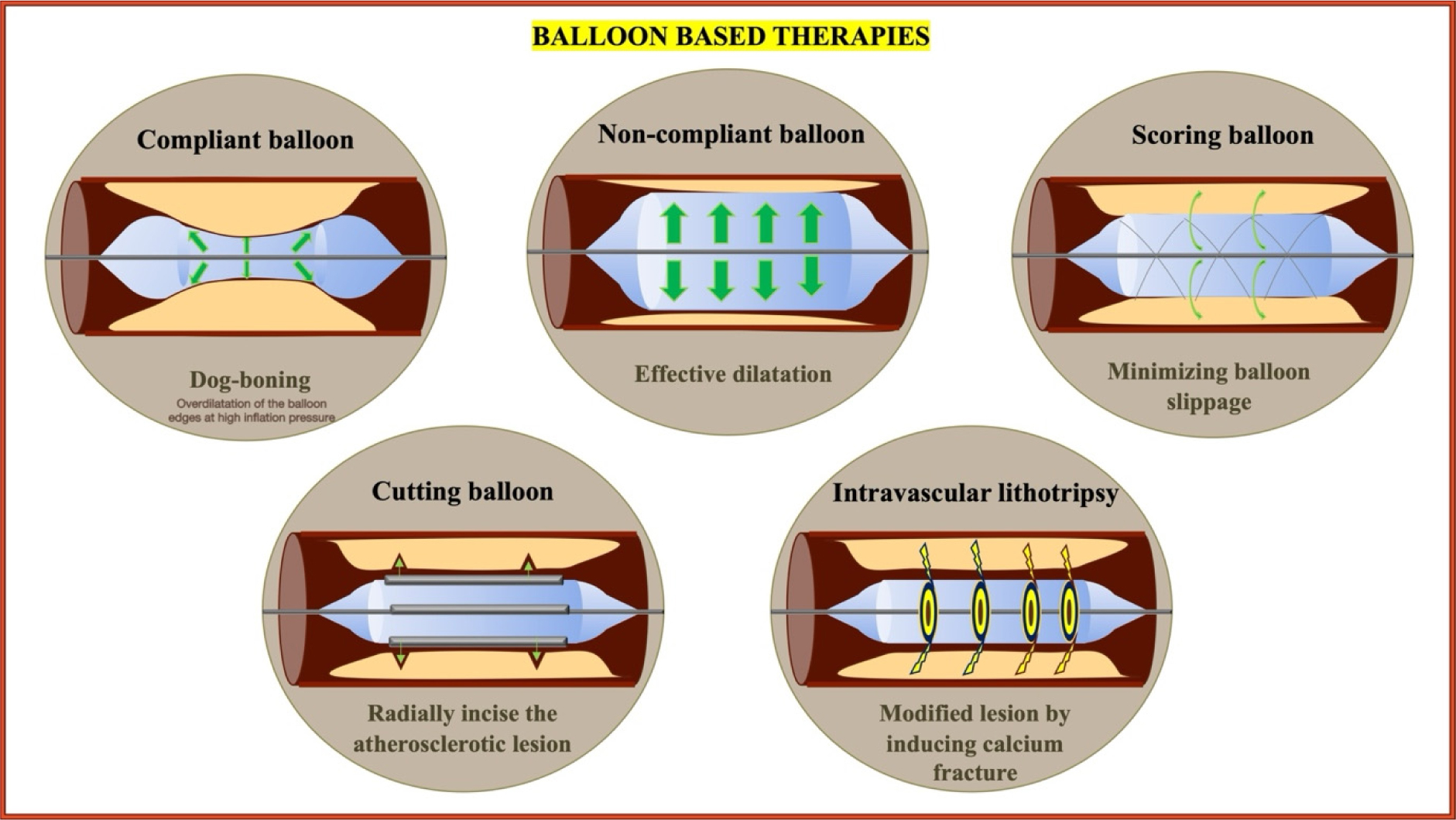
Safian RD, Hoffmann MA, Almany S, et al. (1995) Comparison of coronary angioplasty with compliant and noncompliant balloons (the Angioplasty Compliance Trial). Am J Cardiol 76: 518-520. https://doi.org/10.1016/s0002-9149(99)80143-x
|
| [36] |
Kawase Y, Saito N, Watanabe S, et al. (2014) Utility of a scoring balloon for a severely calcified lesion: bench test and finite element analysis. Cardiovasc Interv Ther 29: 134-139. https://doi.org/10.1007/s12928-013-0232-6
|
| [37] |
Liang B, Gu N (2021) Evaluation of the safety and efficacy of coronary intravascular lithotripsy for treatment of severely calcified coronary stenoses: evidence from the serial disrupt CAD trials. Front Cardiovasc Med 8: 724481. https://doi.org/10.3389/fcvm.2021.724481
|
| [38] |
Basavarajaiah S, Ielasi A, Raja W, et al. (2022) Long-term outcomes following intravascular lithotripsy (IVL) for calcified coronary lesions: a real-world multicenter european study. Catheter Cardiovasc Interv 101: 250-260. https://doi.org/10.1002/ccd.30519
|
| [39] |
Gruslova AB, Inanc IH, Cilingiroglu M, et al. (2024) Review of intravascular lithotripsy for treating coronary, peripheral artery, and valve calcifications. Catheter Cardiovasc Interv 103: 295-307. https://doi.org/10.1002/ccd.30933
|
| [40] |
Kereiakes DJ, Di Mario C, Riley RF, et al. (2021) Intravascular lithotripsy for treatment of calcified coronary lesions: patient-level pooled analysis of the disrupt CAD studies. JACC Cardiovasc Interv 14: 1337-1348. https://doi.org/10.1016/j.jcin.2021.04.015
|
| [41] | Dawood M, Elwany M, Abdelgawad H, et al. (2024) Coronary calcifications, the Achilles heel in coronary interventions. Postepy Kardiol Interwencyjnej 20: 1-17. https://doi.org/10.5114/aic.2024.136415 |
| [42] |
Safian RD, Feldman T, Muller DW, et al. (2001) Coronary angioplasty and Rotablator atherectomy trial (CARAT): immediate and late results of a prospective multicenter randomized trial. Catheter Cardiovasc Interv 53: 213-220. https://doi.org/10.1002/ccd.1151
|
| [43] |
Sharma SK, Tomey MI, Teirstein PS, et al. (2019) North American expert review of rotational atherectomy. Circ Cardiovasc Interv 12: e007448. https://doi.org/10.1161/CIRCINTERVENTIONS.118.007448
|
| [44] |
Abdel-Wahab M, Richardt G, Joachim Büttner H, et al. (2013) High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: the randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv 6: 10-19. https://doi.org/10.1016/j.jcin.2012.07.017
|
| [45] |
Abdel-Wahab M, Toelg R, Byrne RA, et al. (2018) High-speed rotational atherectomy versus modified balloons prior to drug-eluting stent implantation in severely calcified coronary lesions. Circ Cardiovasc Interv 11: e007415. https://doi.org/10.1161/CIRCINTERVENTIONS.118.007415
|
| [46] |
Neumann FJ, Sousa-Uva M, Ahlsson A, et al. (2019) 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J 40: 87-165. https://doi.org/10.1093/eurheartj/ehy394
|
| [47] |
Dill T, Dietz U, Hamm CW, et al. (2000) A randomized comparison of balloon angioplasty versus rotational atherectomy in complex coronary lesions (COBRA study). Eur Heart J 21: 1759-1766. https://doi.org/10.1053/euhj.2000.2242
|
| [48] |
Mankerious N, Richardt G, Allali A, et al. (2024) Lower revascularization rates after high-speed rotational atherectomy compared to modified balloons in calcified coronary lesions: 5-year outcomes of the randomized PREPARE-CALC trial. Clin Res Cardiol 113: 1051-1059. https://doi.org/10.1007/s00392-024-02434-1
|
| [49] |
Florek K, Bartoszewska E, Biegała S, et al. (2023) Rotational atherectomy, orbital atherectomy, and intravascular lithotripsy comparison for calcified coronary lesions. J Clin Med 12: 7246. https://doi.org/10.3390/jcm12237246
|
| [50] |
Redfors B, Sharma SK, Saito S, et al. (2020) Novel micro crown orbital atherectomy for severe lesion calcification. Circ Cardiovasc Interv 13: e008993. https://doi.org/10.1161/CIRCINTERVENTIONS.120.008993
|
| [51] | Shlofmitz E, Shlofmitz R, Lee MS (2019) Orbital atherectomy: a comprehensive review. Interv Cardiol Clin 8: 161-171. https://doi.org/10.1016/j.iccl.2018.11.006 |
| [52] |
Parikh K, Chandra P, Choksi N, et al. (2013) Safety and feasibility of orbital atherectomy for the treatment of calcified coronary lesions: the ORBIT I trial. Catheter Cardiovasc Interv 81: 1134-1139. https://doi.org/10.1002/ccd.24700
|
| [53] |
Chambers JW, Feldman RL, Himmelstein SI, et al. (2014) Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc Interv 7: 510-518. https://doi.org/10.1016/j.jcin.2014.01.158
|
| [54] |
Lee M, Généreux P, Shlofmitz R, et al. (2017) Orbital atherectomy for treating de novo, severely calcified coronary lesions: 3-year results of the pivotal ORBIT II trial. Cardiovasc Revasc Med 18: 261-264. https://doi.org/10.1016/j.carrev.2017.01.011
|
| [55] | Koike J, Iwasaki Y, Sato T, et al. (2023) Acute and mid-term results of percutaneous coronary intervention for severely calcified coronary artery lesions with orbital atherectomy system. J Invasive Cardiol 35. https://doi.org/10.25270/jic/23.00131 |
| [56] |
Rola P, Włodarczak S, Barycki M, et al. (2023) Safety and efficacy of orbital atherectomy in the all-comer population: mid-term results of the Lower Silesian Orbital Atherectomy Registry (LOAR). J Clin Med 12: 5842. https://doi.org/10.3390/jcm12185842
|
| [57] |
Généreux P, Kirtane AJ, Kandzari DE, et al. (2022) Randomized evaluation of vessel preparation with orbital atherectomy prior to drug-eluting stent implantation in severely calcified coronary artery lesions: design and rationale of the ECLIPSE trial. Am Heart J 249: 1-11. https://doi.org/10.1016/j.ahj.2022.03.003
|
| [58] |
Kirtane AJ, Ribichini F (2024) Atherectomy for calcified plaques: orbital for most? Pros and cons. EuroIntervention 20: e627-e629. https://doi.org/10.4244/EIJ-E-24-00014
|
| [59] |
Okamoto N, Egami Y, Nohara H, et al. (2023) Direct comparison of rotational vs orbital atherectomy for calcified lesions guided by optical coherence tomography. JACC Cardiovasc Interv 16: 2125-2136. https://doi.org/10.1016/j.jcin.2023.06.016
|
| [60] |
Shibui T, Tsuchiyama T, Masuda S, et al. (2021) Excimer laser coronary atherectomy prior to paclitaxel-coated balloon angioplasty for de novo coronary artery lesions. Lasers Med Sci 36: 111-117. https://doi.org/10.1007/s10103-020-03019-w
|
| [61] |
Tonomura D, Shimada Y, Yamanaka Y, et al. (2022) Laser vaporization of atherothrombotic burden before drug-coated balloon application in ST-segment elevation myocardial infarction: two-year outcomes of the laser-DCB trial. Catheter Cardiovasc Interv 99: 1758-1765. https://doi.org/10.1002/ccd.30149
|
| [62] |
Doolub G, Ly HQ, Marquis-Gravel G (2024) Should rotational atherectomy be used more often in STEMI to treat calcified culprit lesions?. Can J Cardiol 40: 1234-1236. https://doi.org/10.1016/j.cjca.2024.01.021
|
| [63] |
Hemetsberger R, Mankerious N, Muntané-Carol G, et al. (2024) In-hospital outcomes of rotational atherectomy in ST-elevation myocardial infarction: results from the multicentre ROTA-STEMI network. Can J Cardiol 40: 1226-1233. https://doi.org/10.1016/j.cjca.2023.12.018
|
| [64] |
Shahin M, Candreva A, Siegrist PT (2018) Rotational atherectomy in acute STEMI with heavily calcified culprit lesion is a rule breaking solution. Curr Cardiol Rev 14: 213-216. https://doi.org/10.2174/1573403X14666180523084846
|
| [65] | Błaszkiewicz M, Florek K, Zimoch W, et al. (2024) Predictors of periprocedural myocardial infarction after rotational atherectomy. Postepy Kardiol Interwencyjnej 20: 62-66. https://doi.org/10.5114/aic.2024.137419 |
| [66] |
Riley RF, Henry TD, Mahmud E, et al. (2020) SCAI position statement on optimal percutaneous coronary interventional therapy for complex coronary artery disease. Catheter Cardiovasc Interv 96: 346-362. https://doi.org/10.1002/ccd.28994
|
| [67] |
Räber L, Mintz GS, Koskinas KC, et al. (2018) Clinical use of intracoronary imaging. Part 1: guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J 39: 3281-3300. https://doi.org/10.1093/eurheartj/ehy285
|
Figures(3) / Tables(2)

Bharat Khialani, Sara Malakouti, Sandeep Basavarajah, Leontin Lazar, Sylwia Iwanczyk, Bernardo Cortese. How to identify and prepare calcified lesions safely and effectively[J]. AIMS Medical Science, 2025, 12(2): 171-192. doi: 10.3934/medsci.2025011







 DownLoad:
DownLoad: