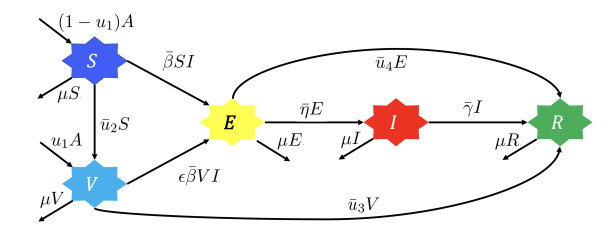
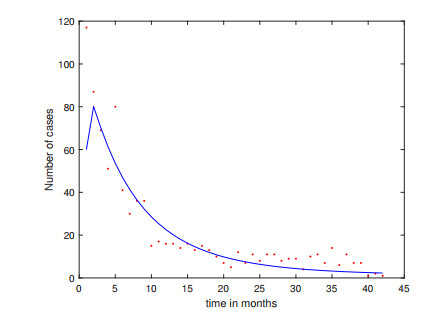
A deterministic model which describes measles' dynamic using newborns and adults first and second dose of vaccination and medical treatment is constructed in this paper. Mathematical analysis about existence of equilibrium points, basic reproduction number, and bifurcation analysis conducted to understand qualitative behaviour of the model. For numerical purposes, we estimated the parameters' values of the model using monthly measles data from Jakarta, Indonesia. Optimal control theory was applied to investigate the optimal strategy in handling measles spread. The results show that all controls succeeded in reducing the number of infected individuals. The cost-effective analysis was conducted to determine the best strategy to reduce number of infected individuals with the lowest cost of intervention. Our result indicates that the use of the first dose measles vaccine with medical treatment is the most optimal strategy to control measles transmission.
Citation: Shinta A. Rahmayani, Dipo Aldila, Bevina D. Handari. Cost-effectiveness analysis on measles transmission with vaccination and treatment intervention[J]. AIMS Mathematics, 2021, 6(11): 12491-12527. doi: 10.3934/math.2021721
A deterministic model which describes measles' dynamic using newborns and adults first and second dose of vaccination and medical treatment is constructed in this paper. Mathematical analysis about existence of equilibrium points, basic reproduction number, and bifurcation analysis conducted to understand qualitative behaviour of the model. For numerical purposes, we estimated the parameters' values of the model using monthly measles data from Jakarta, Indonesia. Optimal control theory was applied to investigate the optimal strategy in handling measles spread. The results show that all controls succeeded in reducing the number of infected individuals. The cost-effective analysis was conducted to determine the best strategy to reduce number of infected individuals with the lowest cost of intervention. Our result indicates that the use of the first dose measles vaccine with medical treatment is the most optimal strategy to control measles transmission.

| [1] |
J. L. Goodson, J. F. Seward, Measles 50 years after use of measles vaccine, Infect. Dis. Clin., 29 (2015), 725–743. doi: 10.1016/j.idc.2015.08.001

|
| [2] | Measles, World Health Organization, 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/measles. |
| [3] | Situasi Campak dan Rubella di Indonesia, Ministry of Health Republic of Indonesia, 2021. Available from: https://pusdatin.kemkes.go.id/download.php?file=download/pusdatin/infodatin/imunisasi%20campak%202018.pdf. |
| [4] | Epidemiology and Prevention of Vaccine-Preventable Diseases, CDC, 2021. Available from: https://www.cdc.gov/vaccines/pubs/pinkbook/index.html. |
| [5] | Measles outbreaks in the Pacific, World Health Organization, 2019. Available from: https://www.who.int/news-room/q-a-detail/measles-outbreaks-in-the-pacific. |
| [6] | A. S. Arliesta, Penatalaksanaan campak. Available from: https://www.alomedika.com/penyakit/pediatri/campak/penatalaksanaan. |
| [7] |
P. A. Stinchfield, W. A. Orenstein, Vitamin a for the management of measles in the United States, Infect. Dis. Clin. Practice, 28 (2020), 181–187. doi: 10.1097/IPC.0000000000000873
|
| [8] | Measles (Rubeola): For Healthcare Professionals, CDC. Available from: https://www.cdc.gov/measles/hcp/index.html. |
| [9] | Measles: Vaccine, World Health Organization. Available from: https://www.who.int/ith/vaccines/measles/en/. |
| [10] |
S. Edward, K. E. Raymond, K. T. Gabriel, F. Nestory, M. G. Godfrey, M. P. Arbogast, A mathematical model for control and elimination of the transmission dynamics of measles, Appl. Comput. Math., 4 (2015), 396–408. doi: 10.11648/j.acm.20150406.12
|
| [11] | Measles – Global situation, World Health Organization, 2019. Available from: https://www.who.int/csr/don/26-november-2019-measles-global_situation/en/. |
| [12] | Immunization Analysis and Insights, World Health Organization. Available from: https://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/active/measles_monthlydata/en/. |
| [13] |
M. Fakhruddin, D. Suandi, S. Sumiati, H. Fahlena, N. Nuraini, E. Soewono, Investigation of a measles transmission with vaccination: A case study in Jakarta, Indonesia, Math. Biosci. Eng., 17 (2020), 2998–3018. doi: 10.3934/mbe.2020170
|
| [14] | E. A. Bakare, Y. A. Adekunle, K. O. Kadiri, Modelling and simulation of the dynamics of the transmission of measles, Int. J. Comput. Trends Technol., 3 (2012), 174–178. |
| [15] | S. Okyere-Siabouh, I. Adetunde, Mathematical model for the study of measles in cape coast metropolis, Int. J. Mod. Biol. Med., 4 (2013), 110–113. |
| [16] | O. M. Tessa, Mathematical model for control of measles by vaccination, Proceedings of Mali Symposium on Applied Sciences, 2006 (2006), 31–36. |
| [17] |
J. Huang, S. Ruan, X. Wu, X. Zhou, Seasonal transmission dynamics of measles in China, Theory Biosci., 137 (2018), 185–195. doi: 10.1007/s12064-018-0271-8
|
| [18] | A. A. Momoh, M. O. Ibrahim, I. J. Uwanta, S. B. Manga, Mathematical model for control of measles epidemiology, Int. J. Pure Appl. Math., 87 (2013), 707–718. |
| [19] | E. M. Musyoki, R. M. Ndungu, S. Osman, A mathematical model for the transmission of measles with passive immunity, Int. J. Res. Math. Stat. Sci., 6 (2019), 1–8. |
| [20] | D. Aldila, D. Asrianti, A deterministic model of measles with imperfect vaccination and quarantine intervention, J. Phys., 1218 (2019), 012044. |
| [21] |
Z. Memon, S. Qureshi, B. R. Memon, Mathematical analysis for a new nonlinear measles epidemiological system using real incidence data from Pakistan, Eur. Phys. J. Plus, 135 (2020), 135. doi: 10.1140/epjp/s13360-020-00219-9
|
| [22] |
R. Almeida, S. Qureshi, A fractional measles model having monotonic real statistical data for constant transmission rate of the disease, Fractal Fractional, 3 (2019), 53. doi: 10.3390/fractalfract3040053
|
| [23] | S. Qureshi, Z. Memon, Monotonically decreasing behavior of measles epidemic well captured by Atangana-Baleanu-Caputo fractional operator under real measles data of Pakistan, Chaos, Solitons Fractals, 131 (2019), 109478. |
| [24] |
S. Qureshi, Real life application of Caputo fractional derivative for measles epidemiological autonomous dynamical system, Chaos, Solitons Fractals, 134 (2020), 109744. doi: 10.1016/j.chaos.2020.109744
|
| [25] |
S. Qureshi, Effects of vaccination on measles dynamics under fractional conformable derivative with Liouville-Caputo operator, Eur. Phys. J. Plus, 135 (2020), 63. doi: 10.1140/epjp/s13360-020-00133-0
|
| [26] |
D. Aldila, Analyzing the impact of the media campaign and rapid testing for COVID-19 as an optimal control problem in East Java, Indonesia, Chaos, Solitons Fractals, 141 (2020), 110364. doi: 10.1016/j.chaos.2020.110364
|
| [27] |
D. Aldila, M. Z. Ndii, B. M. Samiadji, Optimal control on COVID-19 eradication program in Indonesia under the effect of community awareness, Math. Biosci. Eng., 17 (2020), 6355–6389. doi: 10.3934/mbe.2020335
|
| [28] | D. Aldila, B. D. Handari, A. Widyah, G. Hartanti, Strategies of optimal control for HIV spreads prevention with health campaign, Commun. Math. Biol. Neurosci., 2020 (2020), 1–31. |
| [29] |
B. D. Handari, F. Vitra, R. Ahya, S. T. Nadya, D. Aldila, Optimal control in a malaria model: Intervention of fumigation and bed nets, Adv. Differ. Equations, 2019 (2019), 497. doi: 10.1186/s13662-019-2424-6
|
| [30] |
M. Mandal, S. Jana, S. K. Nandi, A. Khatua, S. Adak, T. K. Kar, A model based study on the dynamics of COVID-19: Prediction and control, Chaos, Solitons Fractals, 136 (2020), 109889. doi: 10.1016/j.chaos.2020.109889
|
| [31] | L. Pang, S. Ruan, S. Liu, Z. Zhao, X. Zhang, Transmission dynamics and optimal control of measles epidemics, Appl. Math. Comput., 256 (2015), 131–147. |
| [32] | S. O. Adewale, I. A. Olopade, S. O. Ajao, G. A. Adeniran, Optimal control analysis of the dynamical spread of measles, Int. J. Res., 4 (2016), 169–188. |
| [33] |
H. W. Berhe, O. D. Makinde, Computational modelling and optimal control of measlesepidemic in human population, Biosystems, 190 (2020), 104102. doi: 10.1016/j.biosystems.2020.104102
|
| [34] | M. Ghosh, S. Olaniyi, O. S. Obabiyi, Mathematical analysis of reinfection and relapse in malaria dynamics, Appl. Math. Comput., 373 (2020), 125044. |
| [35] | Jumlah Penduduk Provinsi DKI Jakarta Menurut Kelompok Umur dan Jenis Kelamin, 2018-2019. Available from: https://jakarta.bps.go.id/dynamictable/2019/09/16/58/jumlah-penduduk-provinsi -dki-jakarta-menurut-kelompok-umur-dan-jenis-kelamin-2018-.html. |
| [36] | Indonesia: WHO and UNICEF estimates of immunization coverage: 2019 revision, World Health Organization. Available from: https://www.who.int/immunization/monitoring_surveillance/data/idn.pdf. |
| [37] | Data D K I Jakarta 2018 (Metode Baru), Badan Pusat Statistik. Available from: https://ipm.bps.go.id/data/provinsi/metode/baru/3100. |
| [38] | Measles (Rubeola): Vaccine for Measles, CDC. Available from: https://www.cdc.gov/measles/vaccination.html. |
| [39] |
D. Aldila, H. Seno, A population dynamics model of mosquito-borne disease transmission, focusing on mosquitoes biased distribution and mosquito repellent use, Bull. Math. Biol., 81 (2019), 4977–5008. doi: 10.1007/s11538-019-00666-1
|
| [40] |
K. P. Wijaya, D. Aldila, L. E. Schäfer, Learning the seasonality of disease incidences from empirical data, Ecol. Complex., 38 (2019), 83–97. doi: 10.1016/j.ecocom.2019.03.006
|
| [41] |
D. Aldila, H. Padma, K. Khotimah, B. Desjwiandra, H. Tasman, Analyzing the mers disease control strategy through an optimal control problem, Int. J. Appl. Math. Comput. Sci., 28 (2018), 169–184. doi: 10.2478/amcs-2018-0013
|
| [42] |
T. K. Kar, S. K. Nandi, S. Jana, M. Mandal, Stability and bifurcation analysis of an epidemic model with the effect of media, Chaos, Solitons Fractals, 120 (2019), 188–199. doi: 10.1016/j.chaos.2019.01.025
|
| [43] | F. Agusto, M. Leite, Optimal control and cost-effective analysis of the 2017 meningitis outbreak in nigeria, Infect. Dis. Model., 4 (2019), 161–187. |
| [44] |
O. Diekmann, J. A. P. Heesterbeek, M. G. Roberts, The construction of next-generation matrices for compartmental epidemic models, J. R. Soc. Interface, 7 (2010), 873–885. doi: 10.1098/rsif.2009.0386
|
| [45] |
C. Castillo-Chavez, B. Song, Dynamical models of tuberculosis and their applications, Math. Biosci. Eng., 1 (2004), 361–404. doi: 10.3934/mbe.2004.1.361
|
| [46] | M. Martcheva, An introduction to mathematical epidemiology, Vol. 61, Springer, 2015. |
| [47] | S. Lenhart, J. T. Workman, Optimal control applied to biological models, New York: CRC Press, 2007. |
| [48] | D. Aldila, Cost-effectiveness and backward bifurcation analysis on COVID-19 transmission model considering direct and indirect transmission, Commun. Math. Biol. Neurosci., 2020 (2020), 1–28. |
| [49] |
K. O. Okosun, O. Rachid, N. Marcus, Optimal control strategies and cost-effectiveness analysis of a malaria model, Biosystems, 111 (2013), 83–101. doi: 10.1016/j.biosystems.2012.09.008
|
| [50] |
X. Yang, Generalized form of hurwitz-routh criterion and hopf bifurcation of higher order, Appl. Math. Lett., 15 (2002), 615–621. doi: 10.1016/S0893-9659(02)80014-3
|
| [51] | J. Carr, Applications of center manifold theory, Applied Mathematical Sciences, Springer, 1982. |
| [52] | O. J. Peter, O. A. Afolabi, A. A. Victor, C. E. Akpan, F. A. Oguntolu, Mathematical model for the control of measles, J. Appl. Sci. Env. Manage., 22 (2018), 571–576. |
| [53] | More than 140,000 die from measles as cases surge worldwide, World Health Organization, 2019. Available from: https://www.who.int/news/item/05-12-2019-more-than-140-000-die-from-measles-as-cases-surge-worldwide. |

Figures(21) / Tables(6)

Shinta A. Rahmayani, Dipo Aldila, Bevina D. Handari. Cost-effectiveness analysis on measles transmission with vaccination and treatment intervention[J]. AIMS Mathematics, 2021, 6(11): 12491-12527. doi: 10.3934/math.2021721







 DownLoad:
DownLoad: